

Multicenter epidemiological study to assess the population of CKD patients in Greece: results from the PRESTAR study
- PMID: 25406080
- PMCID: PMC4236082
- DOI: 10.1371/journal.pone.0112767
Multicenter epidemiological study to assess the population of CKD patients in Greece: results from the PRESTAR study
Abstract
Background: Chronic Kidney Disease (CKD) is a relatively common condition not only associated with increased morbidity and mortality but also fuelling End Stage Renal Disease (ESRD). Among developed nations, Greece has one of the highest ESRD incidence rates, yet there is limited understanding of the epidemiology of earlier stages of CKD.
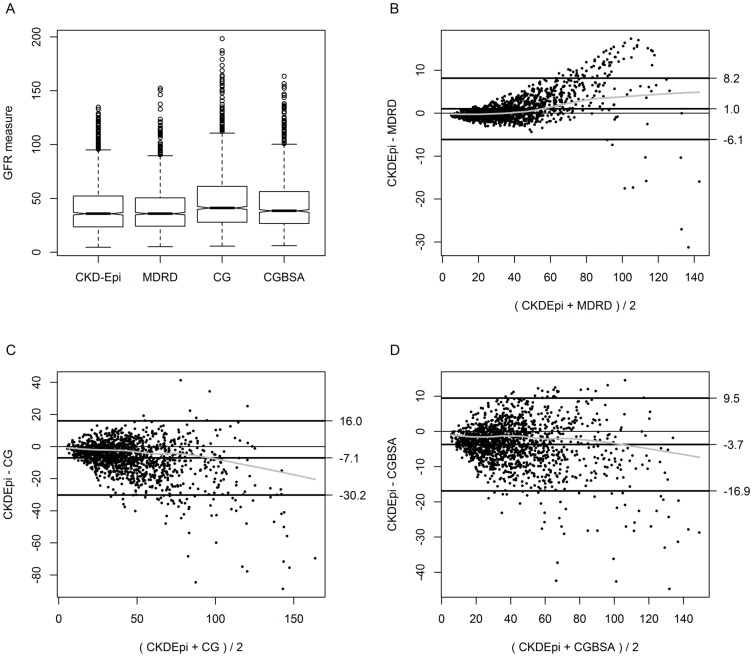
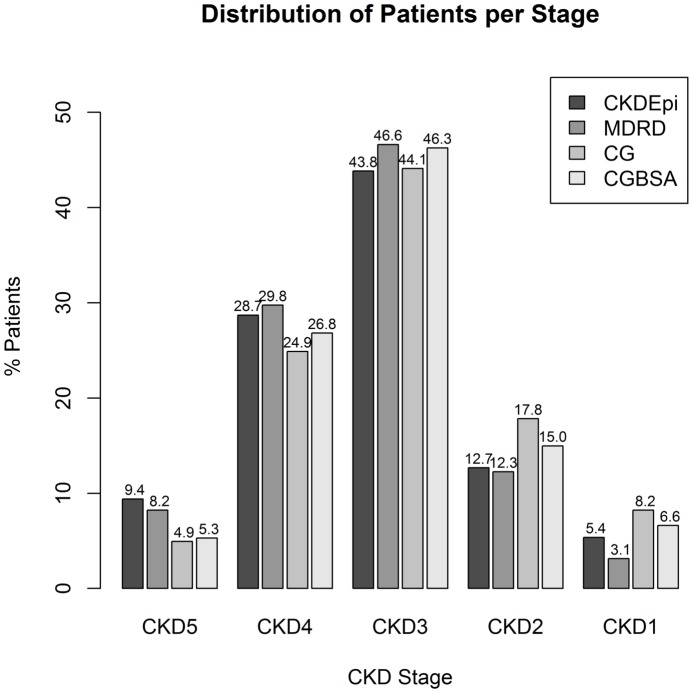
Methods: Cross-sectional survey of pre-dialysis CKD outpatients in nephrology clinics in the National Health Care system between October 2009 and October 2010. Demographics, cause of CKD, blood pressure, level of renal function, duration of CKD and nephrology care, and specialty of referral physician were collected and analyzed. Different methods for estimating renal function (Cockroft-Gault [CG], CKD-Epi and MDRD) and staging CKD were assessed for agreement.
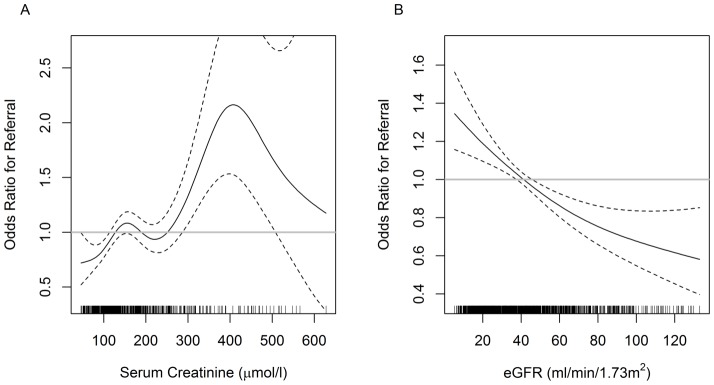
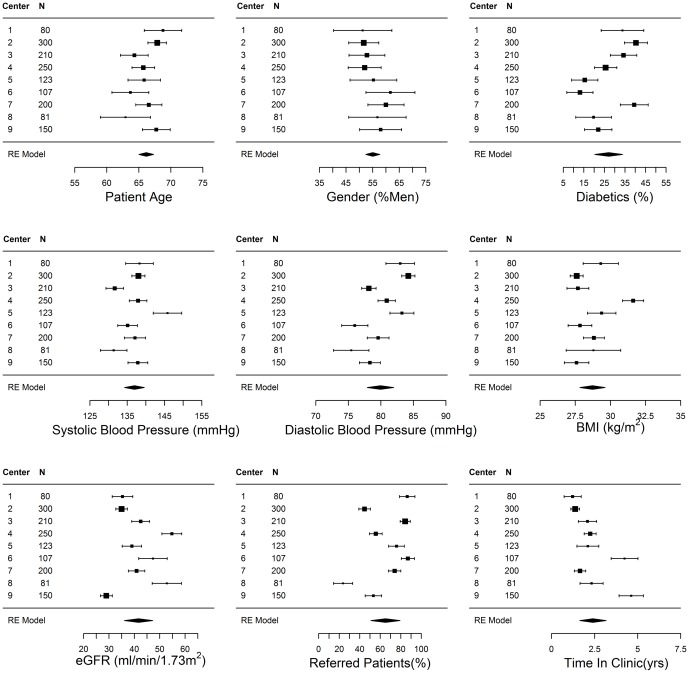
Results: A total of 1,501 patients in 9 centers were enrolled. Diabetic nephropathy was the most common nephrologist assigned cause of CKD (29.7%). In total, 36.5% of patients had self-referred to the nephrologist; patients with diabetes or serum creatinine above 220 µmol/l (eGFR<40 ml/min/1.73 m2) were more likely to have been referred by a physician. Agreement between MDRD and CKD-Epi, but not between CG, the other estimating equations, was excellent. There was substantial heterogeneity with respect to renal diagnoses, referral patterns and blood pressure among participating centers.
Conclusions: In this first epidemiologic assessment of CKD in Greece, we documented delayed referral and high rates of self-referral among patients with CKD. eGFR reporting, currently offered by a limited number of laboratories, may facilitate detection of CKD at an earlier, more treatable stage.
Conflict of interest statement
Figures
References
-
- Locatelli F, Vecchio LD, Pozzoni P (2002) The importance of early detection of chronic kidney disease. Nephrol Dial Transplant 17 Suppl 11: 2–7. - PubMed
-
- Kinchen KS, Sadler J, Fink N, Brookmeyer R, Klag MJ, et al. (2002) The timing of specialist evaluation in chronic kidney disease and mortality. Ann Intern Med 137: 479–486. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
