

Use of a fixed combination of acetylsalicylic acid, acetaminophen and caffeine compared with acetaminophen alone in episodic tension-type headache: meta-analysis of four randomized, double-blind, placebo-controlled, crossover studies
- PMID: 25406671
- PMCID: PMC4256978
- DOI: 10.1186/1129-2377-15-76
Use of a fixed combination of acetylsalicylic acid, acetaminophen and caffeine compared with acetaminophen alone in episodic tension-type headache: meta-analysis of four randomized, double-blind, placebo-controlled, crossover studies
Abstract
Background: Most patients with episodic tension-type headache treat headache episodes with over-the-counter medication. Combination analgesics containing caffeine may be more effective and as well tolerated as monotherapy. The aim of this study was to evaluate the efficacy of the combination of acetylsalicylic acid, acetaminophen (paracetamol) and caffeine in episodic tension-type headache using recently recommended endpoints.
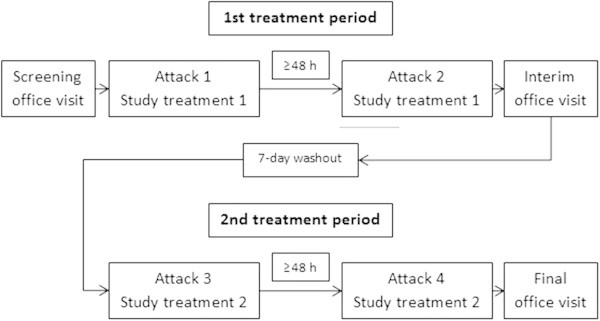
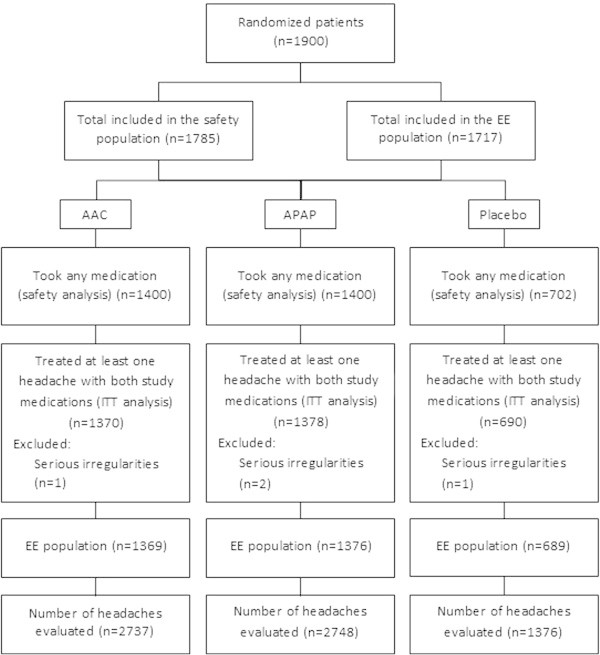
Methods: Four randomized, controlled trials of identical design in 1,900 patients with episodic tension-type headache comparing acetylsalicylic acid, acetaminophen and caffeine vs. acetaminophen or placebo were pooled. Analysis populations were 'all headache episodes' and those with 'severe pain at baseline'. Post-hoc defined primary endpoint: headache episodes pain-free at 2 h. Secondary endpoints: headache episodes pain-free at 1 h, headache response at 2 h (mild or no pain), degree of interference with daily activities.
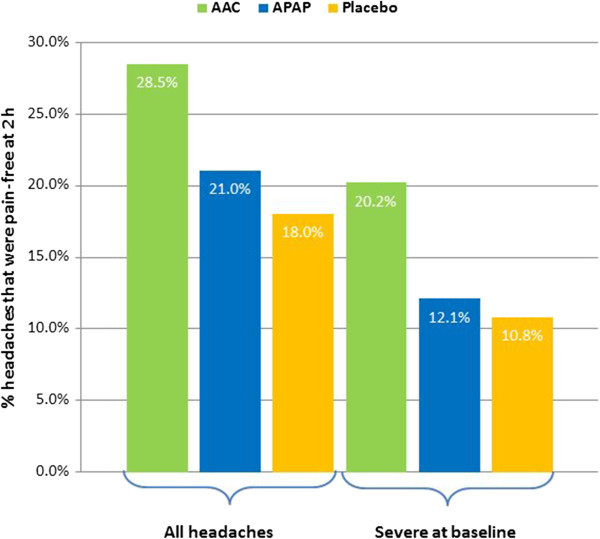
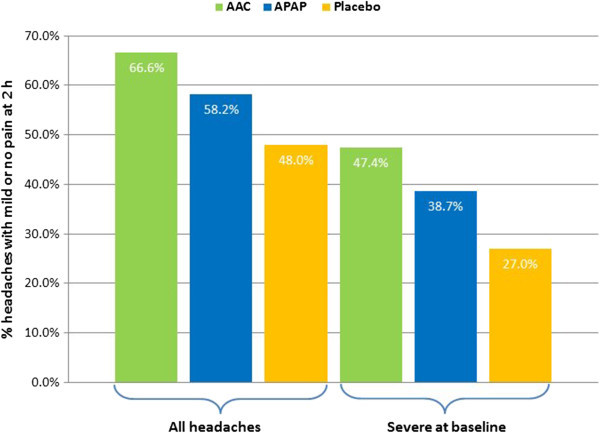
Results: 6,861 headache episodes were treated, including 2,215 severe headache episodes. The proportion of headache episodes pain-free at 2 h was significantly higher with the triple combination (28.5%) vs. acetaminophen (21.0%) and placebo (18.0%) (p < 0.0001), and similarly for those severe at baseline (20.2% vs. 12.1% and 10.8%; p ≤ 0.0003). A similar pattern of superiority was observed for secondary endpoints. The triple combination was generally well tolerated.
Conclusions: The combination of acetylsalicylic acid, acetaminophen and caffeine is effective and well tolerated in episodic tension-type headache, and significantly superior to acetaminophen with regard to being pain-free at 2 h, headache response at 2 h and ability to return to daily activities, even in those with pain rated severe at baseline.
Figures
References
-
- Brennum J, Brinck T, Schriver L, Wanscher B, Soelberg Sorensen P, Tfelt-Hansen P, Olesen J. Sumatriptan has no clinically relevant effect in the treatment of episodic tension-type headache. Eur J Neurol. 1996;3:23–28. doi: 10.1111/j.1468-1331.1996.tb00184.x. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
