

Adrenergic receptor genotype influences heart failure severity and β-blocker response in children with dilated cardiomyopathy
- PMID: 25406899
- PMCID: PMC4298011
- DOI: 10.1038/pr.2014.183
Adrenergic receptor genotype influences heart failure severity and β-blocker response in children with dilated cardiomyopathy
Abstract
Background: Adrenergic receptor (ADR) genotypes are associated with heart failure (HF) and β-blocker response in adults. We assessed the influence of ADR genotypes in children with dilated cardiomyopathy (DCM).
Methods: Ninety-one children with advanced DCM and 44 with stable DCM were genotyped for three ADR genotypes associated with HF risk in adults: α2cdel322-325, β1Arg389, and β2Arg16. Data were analyzed by genotype and β-blocker use. Mean age at enrollment was 8.5 y.
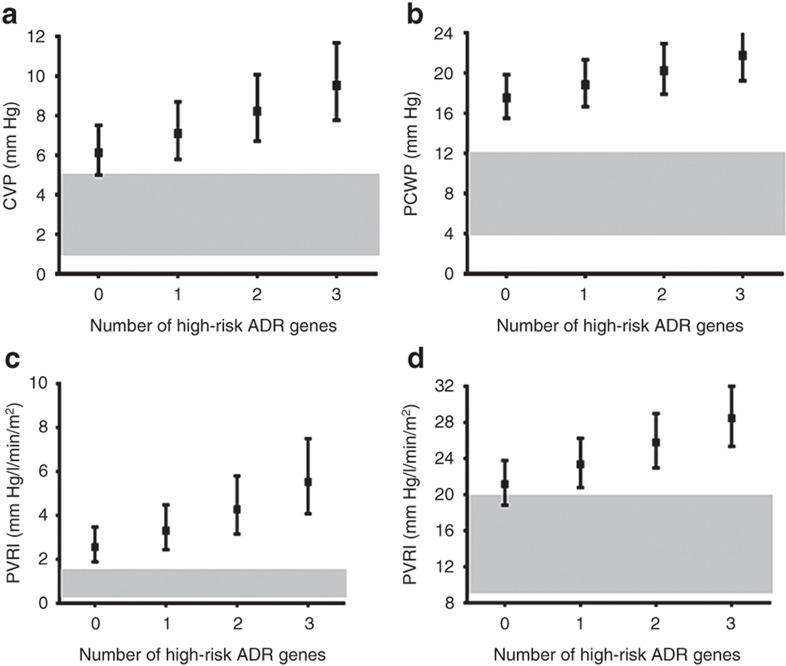
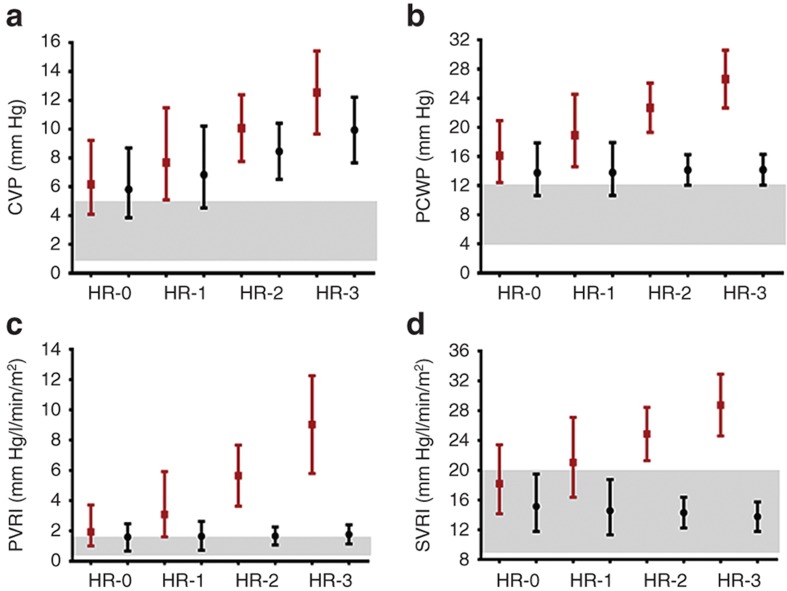
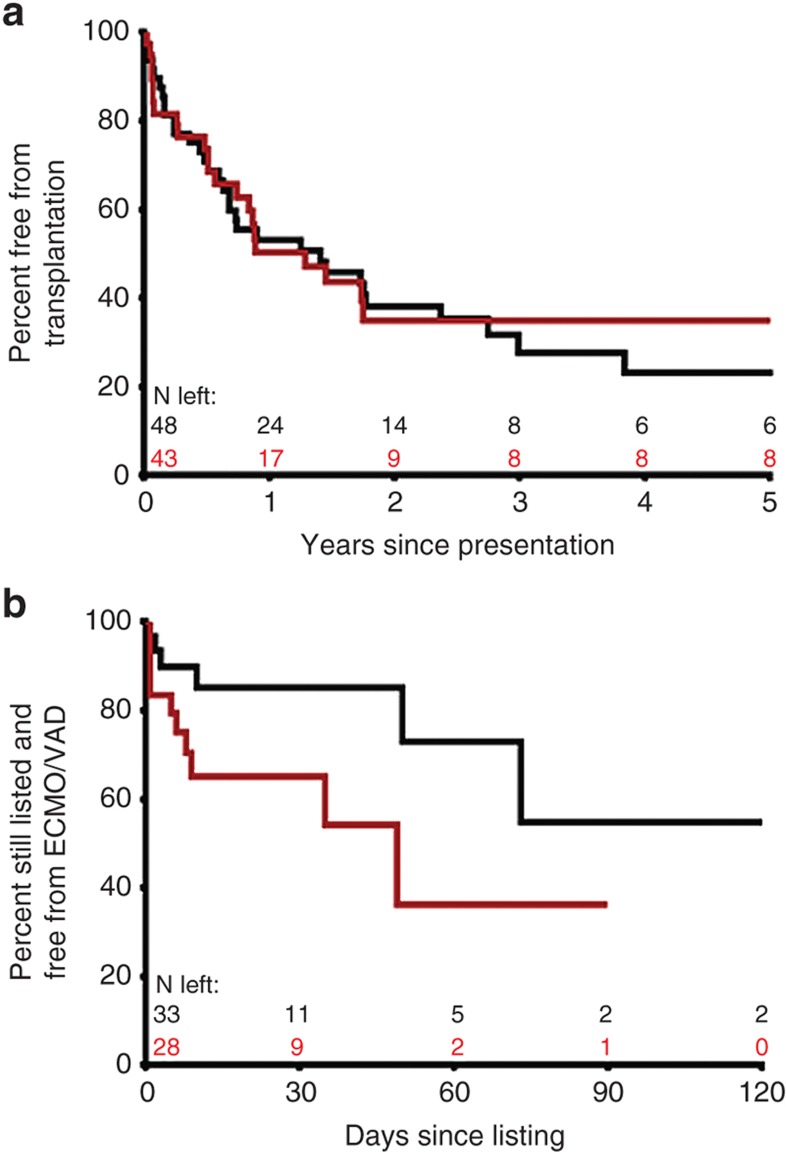
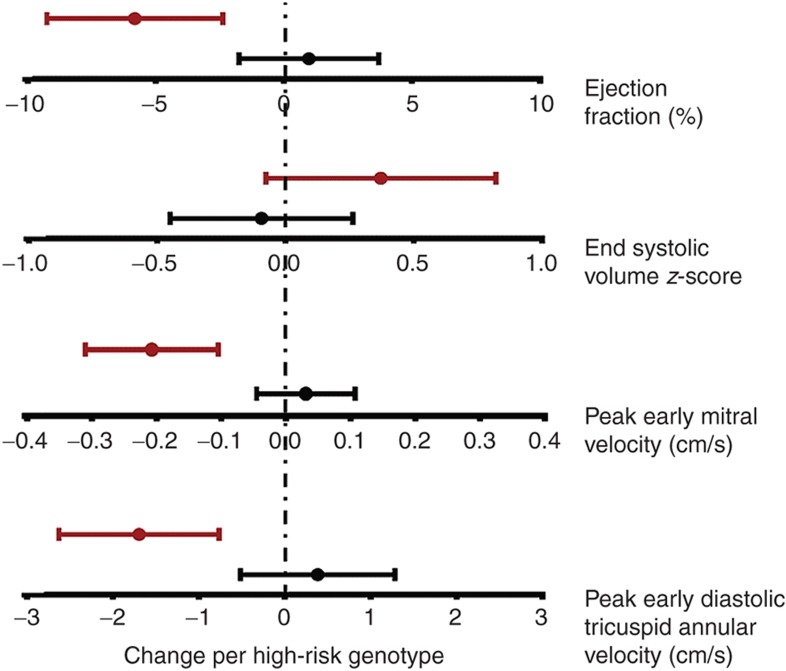
Results: One-year event-free survival was 51% in advanced and 80% in stable DCM. High-risk genotypes were associated with higher left ventricular (LV) filling pressures, higher systemic and pulmonary vascular resistance, greater decline in LV ejection fraction (P < 0.05), and a higher frequency of mechanical circulatory support while awaiting transplant (P = 0.05). While β-blockers did not reduce HF severity in the overall cohort, in the subset with multiple high-risk genotypes, those receiving β-blockers showed better preservation of cardiac function and hemodynamics compared with those not receiving β-blockers (interaction P < 0.05).
Conclusion: Our study identifies genetic risk markers that may help in the identification of patients at risk for developing decompensated HF and who may benefit from early institution of β-blocker therapy before progression to decompensated HF.
Figures
References
-
- Majewski H. Modulation of noradrenaline release through activation of presynaptic beta-adrenoreceptors. J Auton Pharmacol. 1983;3:47–60. - PubMed
-
- Hein L, Kobilka BK. Adrenergic receptor signal transduction and regulation. Neuropharmacology. 1995;34:357–66. - PubMed
-
- Kaye DM, Smirk B, Finch S, Williams C, Esler MD. Interaction between cardiac sympathetic drive and heart rate in heart failure: modulation by adrenergic receptor genotype. J Am Coll Cardiol. 2004;44:2008–15. - PubMed
-
- Small KM, Wagoner LE, Levin AM, Kardia SL, Liggett SB. Synergistic polymorphisms of beta1- and alpha2C-adrenergic receptors and the risk of congestive heart failure. N Engl J Med. 2002;347:1135–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
