

Tonsillectomy or adenotonsillectomy versus non-surgical treatment for chronic/recurrent acute tonsillitis
- PMID: 25407135
- PMCID: PMC7075105
- DOI: 10.1002/14651858.CD001802.pub3
Tonsillectomy or adenotonsillectomy versus non-surgical treatment for chronic/recurrent acute tonsillitis
Abstract
Background: Surgical removal of the tonsils, with or without adenoidectomy (adeno-/tonsillectomy), is a common ENT operation, but the indications for surgery are controversial. This is an update of a Cochrane review first published in The Cochrane Library in Issue 3, 1999 and previously updated in 2009.
Objectives: To assess the effectiveness of tonsillectomy (with and without adenoidectomy) in children and adults with chronic/recurrent acute tonsillitis in reducing the number and severity of episodes of tonsillitis or sore throat.
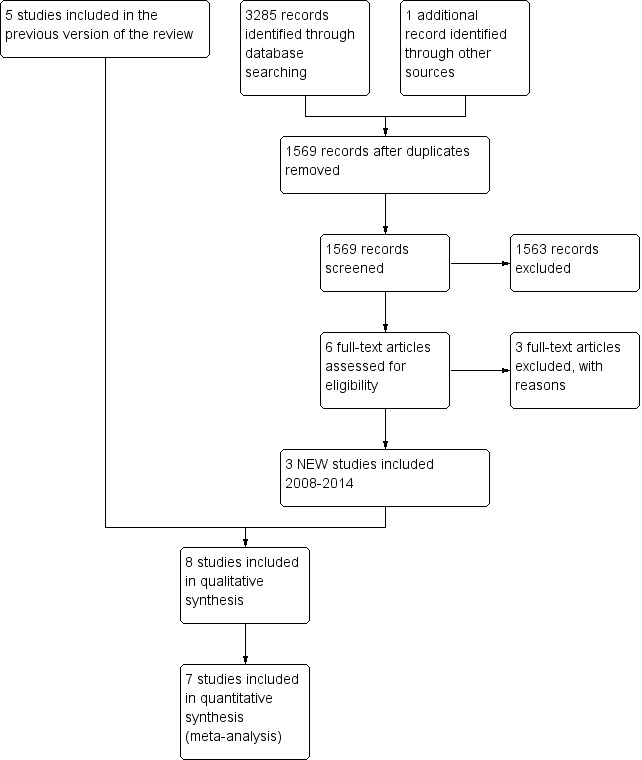
Search methods: We searched the Cochrane Ear, Nose and Throat Disorders Group Trials Register; the Cochrane Central Register of Controlled Trials (CENTRAL); PubMed; EMBASE; CINAHL; Web of Science; Cambridge Scientific Abstracts; ISRCTN and additional sources for published and unpublished trials. The date of the most recent search was 30 June 2014.
Selection criteria: Randomised controlled trials comparing tonsillectomy (with or without adenoidectomy) with non-surgical treatment in adults and children with chronic/recurrent acute tonsillitis.
Data collection and analysis: We used the standard methodological procedures expected by The Cochrane Collaboration.
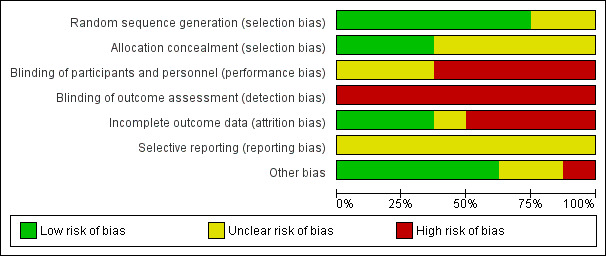
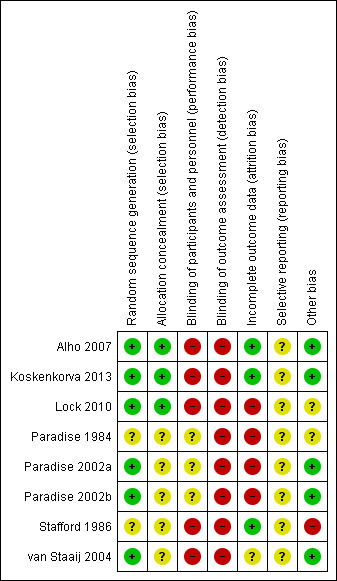
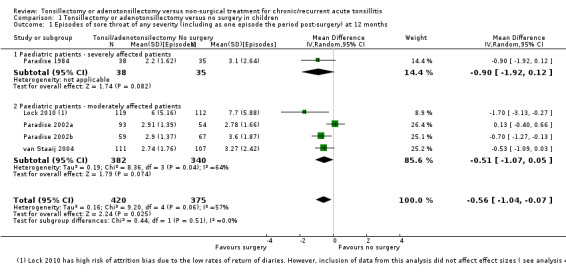
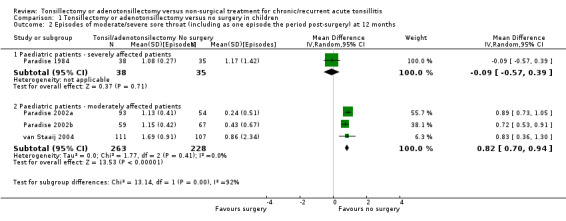
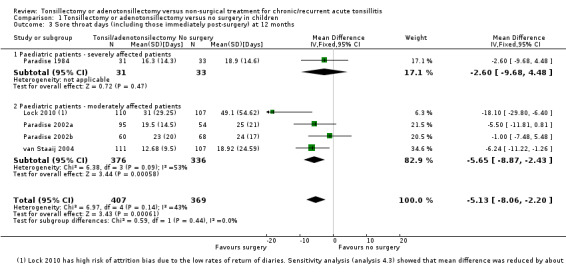
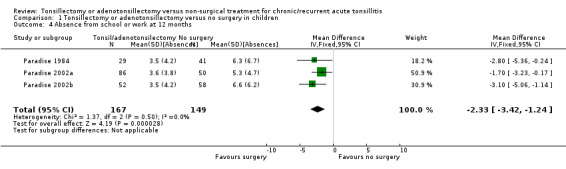
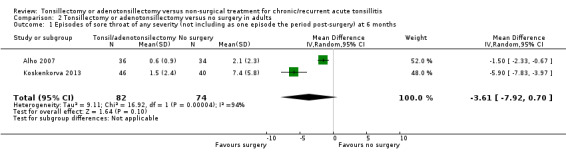
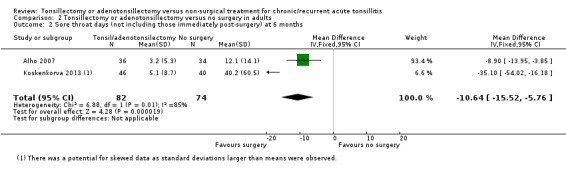
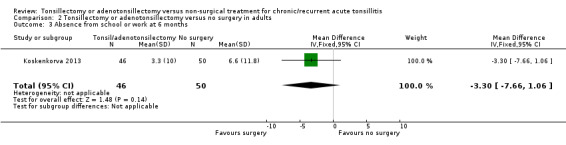
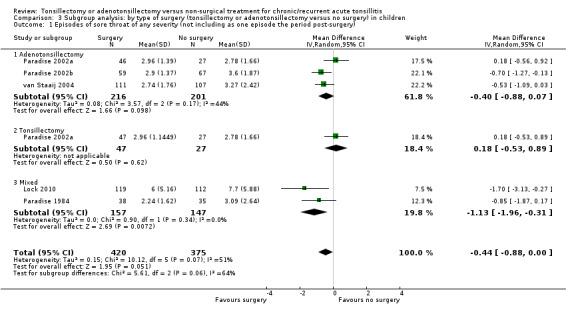
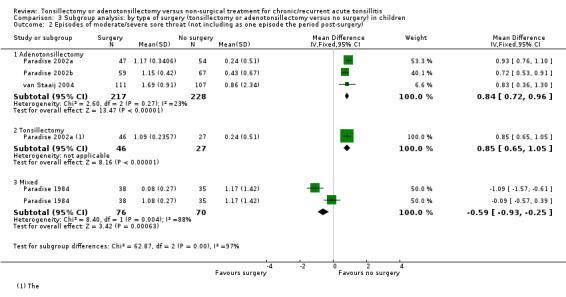
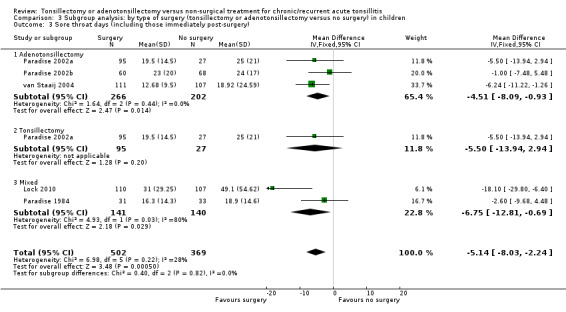
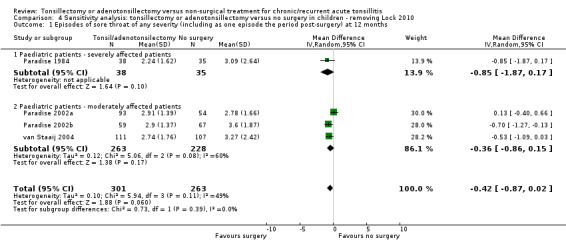
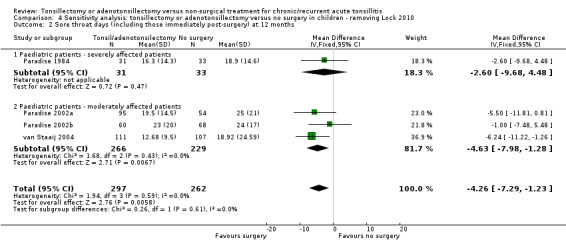
Main results: This review includes seven trials with low to moderate risk of bias: five undertaken in children (987 participants) and two in adults (156 participants). An eighth trial in adults (40 participants) was at high risk of bias and did not provide any data for analysis. Good information about the effectiveness of adeno-/tonsillectomy is only available for the first year following surgery in children and for a shorter period (five to six months) in adults.We combined data from five trials in children; these trials included children who were 'severely affected' (based on the specific 'Paradise' criteria) and less severely affected. Children who had an adeno-/tonsillectomy had an average of three episodes of sore throats (of any severity) in the first postoperative year, compared to 3.6 episodes in the control group; a difference of 0.6 episodes (95% confidence interval (CI) -1 to -0.1; moderate quality evidence). One of the three episodes in the surgical group was the 'predictable' one that occurred in the immediate postoperative period.When we analysed only episodes of moderate/severe sore throat, children who had been more severely affected and had adeno-/tonsillectomy had on average 1.1 episodes of sore throat in the first postoperative year, compared with 1.2 episodes in the control group (low quality evidence). This is not a significant difference but one episode in the surgical group was that occurring immediately after surgery.Less severely affected children had more episodes of moderate/severe sore throat after surgery (1.2 episodes) than in the control group (0.4 episodes: difference 0.8, 95% CI 0.7 to 0.9), but again one episode was the predictable postoperative episode (moderate quality evidence).Data on the number of sore throat days is only available for moderately affected children and is consistent with the data on episodes. In the first year after surgery children undergoing surgery had an average of 18 days of sore throat (of which some - between five and seven on average - will be in the immediate postoperative period), compared with 23 days in the control group (difference 5.1 days, 95% CI 2.2 to 8.1; moderate quality evidence).When we pooled the data from two studies in adults (156 participants), there were 3.6 fewer episodes (95% CI 7.9 fewer to 0.70 more; low quality evidence) in the group receiving surgery within six months post-surgery. However, statistical heterogeneity was significant. The pooled mean difference for number of days with sore throat in a follow-up period of about six months was 10.6 days fewer in favour of the group receiving surgery (95% CI 5.8 fewer to 15.8 fewer; low quality evidence). However, there was also significant statistical heterogeneity in this analysis and the number of days with postoperative pain (which appeared to be on average 13 to 17 days in the two trials) was not included. Given the short duration of follow-up and the differences between studies, we considered the evidence for adults to be of low quality.Two studies in children reported that there was "no statistically significant difference" in quality of life outcomes, but the data could not be pooled. One study reported no difference in analgesics consumption. We found no evidence for prescription of antibiotics.Limited data are available from the included studies to quantify the important risks of primary and secondary haemorrhage.
Authors' conclusions: Adeno-/tonsillectomy leads to a reduction in the number of episodes of sore throat and days with sore throat in children in the first year after surgery compared to (initial) non-surgical treatment. Children who were more severely affected were more likely to benefit as they had a small reduction in moderate/severe sore throat episodes. The size of the effect is very modest, but there may be a benefit to knowing the precise timing of one episode of pain lasting several days - it occurs immediately after surgery as a direct consequence of the procedure. It is clear that some children get better without any surgery, and that whilst removing the tonsils will always prevent 'tonsillitis', the impact of the procedure on 'sore throats' due to pharyngitis is much less predictable.Insufficient information is available on the effectiveness of adeno-/tonsillectomy versus non-surgical treatment in adults to draw a firm conclusion.The impact of surgery, as demonstrated in the included studies, is modest. Many participants in the non-surgical group improve spontaneously (although some people randomised to this group do in fact undergo surgery). The potential 'benefit' of surgery must be weighed against the risks of the procedure as adeno-/tonsillectomy is associated with a small but significant degree of morbidity in the form of primary and secondary haemorrhage and, even with good analgesia, is particularly uncomfortable for adults.
Conflict of interest statement
None known.
Figures
Update of
-
Tonsillectomy or adeno-tonsillectomy versus non-surgical treatment for chronic/recurrent acute tonsillitis.Cochrane Database Syst Rev. 2009 Jan 21;(1):CD001802. doi: 10.1002/14651858.CD001802.pub2. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2014 Nov 19;(11):CD001802. doi: 10.1002/14651858.CD001802.pub3. PMID: 19160201 Updated.
Comment in
-
Tonsillectomy or adenotonsillectomy reduces the number of sore throats in children; however, insufficient information is available on the effectiveness in adults.Evid Based Med. 2015 Apr;20(2):64. doi: 10.1136/ebmed-2014-110153. Epub 2015 Mar 3. Evid Based Med. 2015. PMID: 25736043 No abstract available.
References
References to studies included in this review
Alho 2007 {published data only}
Koskenkorva 2013 {published data only}
-
- Koskenkorva T, Koivunen P, Koskela M, Niemela O, Kristo A, Alho OP. Short‐term outcomes of tonsillectomy in adult patients with recurrent pharyngitis: a randomized controlled trial. CMAJ: Canadian Medical Association Journal 2013;185(8):E331‐6. [DOI: 10.1503/cmaj.121852; PUBMED: 23549975] - DOI - PMC - PubMed
Lock 2010 {published data only}
-
- Lock C, Wilson J, Steen N, Eccles M, Mason H, Carrie S, et al. North of England and Scotland Study of Tonsillectomy and Adeno‐tonsillectomy in Children (NESSTAC): a pragmatic randomised controlled trial with a parallel non‐randomised preference study. Health Technology Assessment 2010;14(13):1‐164, iii‐iv. [DOI: 10.3310/hta14130] - DOI - PubMed
-
- Wilson JA, Steen IN, Lock CA, Eccles MP, Carrie S, Clarke R, et al. Tonsillectomy: a cost‐effective option for childhood sore throat? Further analysis of a randomized controlled trial. Otolaryngology ‐ Head and Neck Surgery 2010;146:122‐8. - PubMed
Paradise 1984 {published data only}
-
- Paradise JL, Bluestone CD, Bachman RZ, Colborn DK, Bernard BS, Taylor FH, et al. Efficacy of tonsillectomy for recurrent throat infection in severely affected children. New England Journal of Medicine 1984;310(11):674‐83. [PUBMED: 6700642] - PubMed
Paradise 2002a {published data only}
-
- Paradise JL, Bluestone CD, Colborn DK, Bernard BS, Rockette HE, Kurs‐Lasky M. Tonsillectomy and adenotonsillectomy for recurrent throat infection in moderately affected children. Pediatrics 2002;110(1 (Pt 1)):7‐15. [PUBMED: 12093941] - PubMed
Paradise 2002b {published data only}
-
- Paradise JL, Bluestone CD, Colborn DK, Bernard BS, Rockette HE, Kurs‐Lasky M. Tonsillectomy and adenotonsillectomy for recurrent throat infection in moderately affected children. Pediatrics 2002;110(1 (Pt 1)):7‐15. [PUBMED: 12093941] - PubMed
Stafford 1986 {published data only}
-
- Stafford N, Haacke N, Sene A, Croft C. The treatment of recurrent tonsillitis in adults. Journal of Laryngology and Otology 1986;100(2):175‐7. [PUBMED: 3950480] - PubMed
van Staaij 2004 {published and unpublished data}
-
- Staaij BK, Akker EH, Rovers MM, Hordijk GJ, Hoes AW, Schilder AG. Effectiveness of adenotonsillectomy in children with mild symptoms of throat infections or adenotonsillar hypertrophy: open, randomised controlled trial. Clinical Otolaryngology 2005;30(1):60‐3. [PUBMED: 15748193] - PubMed
References to studies excluded from this review
Clayburgh 2011 {published data only}
-
- Clayburgh D, Milczuk H, Gorsek S, Sinden N, Bowman K, MacArthur C. Efficacy of tonsillectomy for pediatric patients with dysphagia and tonsillar hypertrophy. Archives of Otolaryngology ‐‐ Head and Neck Surgery 2011;137:1197‐202. - PubMed
Kaiser 1930 {published data only}
-
- Kaiser AD. Results of tonsillectomy. A comparative study of twenty‐two hundred tonsillectomized children with an equal number of controls three and ten years after operation. Journal of the American Medical Association 1930;95:837‐42.
Mawson 1967 {published data only}
-
- Mawson SR, Adlington P, Evans M. A controlled study evaluation of adeno‐tonsillectomy in children. Journal of Laryngology and Otology 1967;81:777‐90. - PubMed
-
- Mawson SR, Adlington P, Evans M. A controlled study evaluation of adeno‐tonsillectomy in children. Journal of Laryngology and Otology 1967;82:963‐79. - PubMed
McKee 1963 {published data only}
Naiboğlu 2010 {published data only}
-
- Naiboğlu B, Külekçi S, Kalaycık C, Sheidaei S, Toros SZ, Egeli E. Improvement in quality of life by adenotonsillectomy in children with adenotonsillar disease. Clinical Otolaryngology 2010;35:383‐9. - PubMed
Roydhouse 1970 {published data only}
-
- Roydhouse N. A controlled study of adenotonsillectomy. Archives of Otolaryngology 1970;92:611‐6. - PubMed
Stalfors 2012 {published data only}
-
- Stalfors J, Ericsson E, Hemlin C, Hultcrantz E, Månsson I, Roos K, et al. Tonsil surgery efficiently relieves symptoms: analysis of 54 696 patients in the National Tonsil Surgery Register in Sweden. Acta Oto‐Laryngologica 2012;132:533‐9. - PubMed
References to ongoing studies
NATTINA 2014 {published data only}
-
- HTA ‐ 12/146/06: The NAtional Trial of Tonsillectomy IN Adults (NATTINA): a clinical and cost effectiveness study. http://www.nets.nihr.ac.uk/projects/hta/1214606. - PMC - PubMed
Additional references
Ashworth 2004
-
- Ashworth M, Latinovic R, Charlton J, Cox K, Rowlands G, Gulliford M. Why has antibiotic prescribing for respiratory illness declined in primary care? A longitudinal study using the General Practice Research Database. Journal of Public Health (Oxford) 2004;26:268–74. - PubMed
Barraclough 2014
-
- Barraclough J, Anari S. Tonsillectomy for recurrent sore throats in children: indications, outcomes, and efficacy. Otolaryngology ‐ Head and Neck Surgery 2014;150:722‐9. - PubMed
Baugh 2011
-
- Baugh RF, Archer SM, Mitchell RB, Rosenfeld RM, Amin R, Burns JJ, et al. Clinical practice guideline: tonsillectomy in children. Otolaryngology ‐ Head and Neck Surgery 2011;144:S1‐30. - PubMed
Blackshaw 2014
Brown 2005
-
- Brown P, Ryan R, Yung M, et al. National Prospective Tonsillectomy Audit. http://www.rcseng.ac.uk/publications/docs/national_prospective.html/view... 2005:1‐40.
Handbook 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions version 5.1.0 [updated March2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Marshall 1998
Paradise 1996
-
- Paradise JL. Tonsillectomy and adenoidectomy. In: Bluestone CD, Stool SE, Kenna MA editor(s). Pediatric Otolaryngology. 3rd Edition. Philadelphia: WB Saunders, 1996:1054‐65.
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Robinson 1996
-
- Robinson K, Gatehouse S, Browning GG. Measuring patient benefit from otorhinolaryngological surgery and therapy. Annals of Otology, Rhinology and Laryngology 1996;105:415‐22. - PubMed
SIGN 2010
-
- Scottish Intercollegiate Guidelines Network ‐ Guideline 117 ‐ Management of sore throat and indications for tonsillectomy ‐ April 2010. www.sign.ac.uk/pdf/sign117.pdf.
Venekamp 2014
References to other published versions of this review
Burton 1999
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous