

Racial/Ethnic Differences in Sleep Disturbances: The Multi-Ethnic Study of Atherosclerosis (MESA)
- PMID: 25409106
- PMCID: PMC4434554
- DOI: 10.5665/sleep.4732
Racial/Ethnic Differences in Sleep Disturbances: The Multi-Ethnic Study of Atherosclerosis (MESA)
Abstract
Objectives: There is limited research on racial/ethnic variation in sleep disturbances. This study aimed to quantify the distributions of objectively measured sleep disordered breathing (SDB), short sleep duration, poor sleep quality, and self-reported sleep disturbances (e.g., insomnia) across racial/ethnic groups.
Design: Cross-sectional study.
Setting: Six US communities.
Participants: Racially/ethnically diverse men and women aged 54-93 y in the Multi-Ethnic Study of Atherosclerosis Sleep Cohort (n = 2,230).
Interventions: N/A.
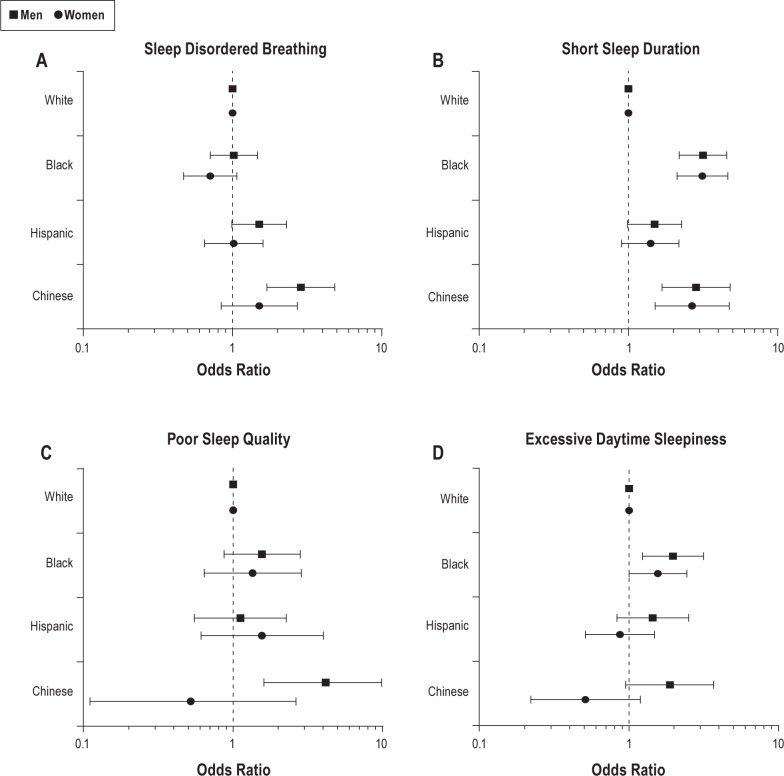
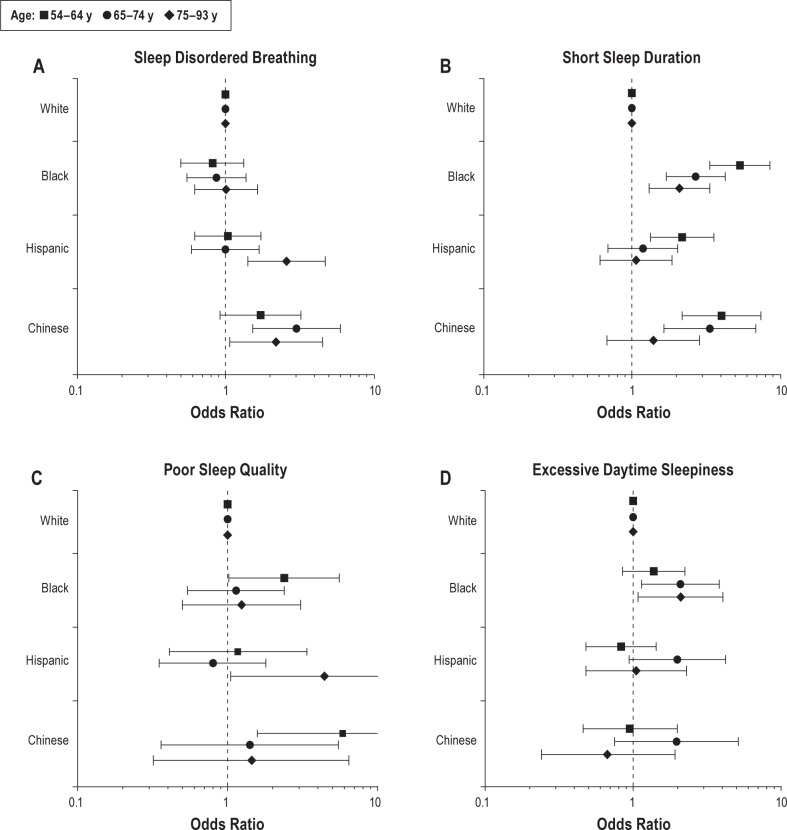
Measurements and results: Information from polysomnography-measured SDB, actigraphy-measured sleep duration and quality, and self-reported daytime sleepiness were obtained between 2010 and 2013. Overall, 15.0% of individuals had severe SDB (apnea-hypopnea index [AHI] ≥ 30); 30.9% short sleep duration (< 6 h); 6.5% poor sleep quality (sleep efficiency < 85%); and 13.9% had daytime sleepiness. Compared with Whites, Blacks had higher odds of sleep apnea syndrome (AHI ≥ 5 plus sleepiness) (sex-, age-, and study site-adjusted odds ratio [OR] = 1.78, 95% confidence interval [CI]: 1.20, 2.63), short sleep (OR = 4.95, 95% CI: 3.56, 6.90), poor sleep quality (OR = 1.57, 95% CI: 1.00, 2.48), and daytime sleepiness (OR = 1.89, 95% CI: 1.38, 2.60). Hispanics and Chinese had higher odds of SDB and short sleep than Whites. Among non-obese individuals, Chinese had the highest odds of SDB compared to Whites. Only 7.4% to 16.2% of individuals with an AHI ≥ 15 reported a prior diagnosis of sleep apnea.
Conclusions: Sleep disturbances are prevalent among middle-aged and older adults, and vary by race/ethnicity, sex, and obesity status. The high prevalence of sleep disturbances and undiagnosed sleep apnea among racial/ethnic minorities may contribute to health disparities.
Keywords: apnea-hypopnea index; body mass index; daytime sleepiness; obesity; polysomnography; race/ethnicity; sleep disordered breathing; sleep disturbance; sleep duration; sleep quality.
© 2015 Associated Professional Sleep Societies, LLC.
Figures

References
-
- Redline S, Foody J. Sleep disturbances: time to join the top 10 potentially modifiable cardiovascular risk factors? Circulation. 2011;124:2049–51. - PubMed
-
- Kripke DF, Garfinkel L, Wingard DL, Klauber MR, Marler MR. Mortality associated with sleep duration and insomnia. Arch Gen Psychiatry. 2002;59:131–6. - PubMed
Publication types
MeSH terms
Grants and funding
- 3R01HL115941-01S1/HL/NHLBI NIH HHS/United States
- R01 HL109493/HL/NHLBI NIH HHS/United States
- 1U34HL105277-01/HL/NHLBI NIH HHS/United States
- R01 HL098433/HL/NHLBI NIH HHS/United States
- 1R01HL083075-01/HL/NHLBI NIH HHS/United States
- 1R01HL113338-01/HL/NHLBI NIH HHS/United States
- P20NS076965/NS/NINDS NIH HHS/United States
- N01-HC-95169/HC/NHLBI NIH HHS/United States
- R01 HL098433-02S1/HL/NHLBI NIH HHS/United States
- R01HL098433/HL/NHLBI NIH HHS/United States
- UL1 TR000170/TR/NCATS NIH HHS/United States
- 1R01HL110068-01A1/HL/NHLBI NIH HHS/United States
- R21 HL108226/HL/NHLBI NIH HHS/United States
- 8UL1TR000170-07/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
