

CASPER plus (CollAborative care in Screen-Positive EldeRs with major depressive disorder): study protocol for a randomised controlled trial
- PMID: 25409776
- PMCID: PMC4247639
- DOI: 10.1186/1745-6215-15-451
CASPER plus (CollAborative care in Screen-Positive EldeRs with major depressive disorder): study protocol for a randomised controlled trial
Erratum in
-
Erratum to: CASPER plus (CollAborative care in screen-positive EldeRs with major depressive disorder): study protocol for a randomised controlled trial.Trials. 2016 Apr 27;17(1):217. doi: 10.1186/s13063-016-1361-x. Trials. 2016. PMID: 27121377 Free PMC article. No abstract available.
Abstract
Background: Depression accounts for the greatest disease burden of all mental health disorders, contributes heavily to healthcare costs, and by 2020 is set to become the second largest cause of global disability. Although 10% to 16% of people aged 65 years and over are likely to experience depressive symptoms, the condition is under-diagnosed and often inadequately treated in primary care. Later-life depression is associated with chronic illness and disability, cognitive impairment and social isolation. With a progressively ageing population it becomes increasingly important to refine strategies to identity and manage depression in older people. Currently, management may be limited to the prescription of antidepressants where there may be poor concordance; older people may lack awareness of psychosocial interventions and general practitioners may neglect to offer this treatment option.
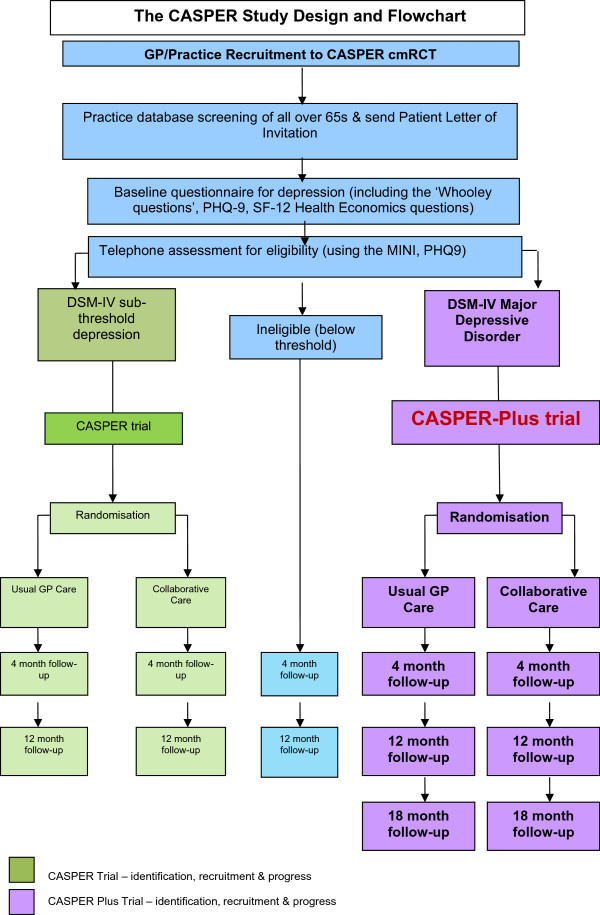
Methods/design: CASPER Plus is a multi-centre, randomised controlled trial of a collaborative care intervention for individuals aged 65 years and over experiencing moderate to severe depression. Selected practices in the North of England identify potentially eligible patients and invite them to participate in the study. A diagnostic interview is carried out and participants with major depressive disorder are randomised to either collaborative care or usual care. The recruitment target is 450 participants. The intervention, behavioural activation and medication management in a collaborative care framework, has been adapted to meet the complex needs of older people. It is delivered over eight to 10 weekly sessions by a case manager liaising with general practitioners. The trial aims to evaluate the clinical and cost effectiveness of collaborative care in addition to usual GP care versus usual GP care alone. The primary clinical outcome, depression severity, will be measured with the Patient Health Questionnaire-9 (PHQ-9) at baseline, 4, 12 and 18 months. Cost effectiveness analysis will assess health-related quality of life using the SF-12 and EQ-5D and will examine cost-consequences of collaborative care. A qualitative process evaluation will be undertaken to explore acceptability, gauge the extent to which the intervention is implemented and to explore sustainability beyond the clinical trial.
Discussion: Results will add to existing evidence and a positive outcome may lead to the commissioning of this model of service in primary care.
Trial registration: ISRCTN45842879 (24 July 2012).
Figures
References
-
- Murray CJ, Lopez AD. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Disease, Injuries and Risk Factors in 1990. Boston, MA: Harvard School of Public Health on behalf of the World Bank; 1996.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
