

Fibro-osseous lesions of the craniofacial skeleton: an update
- PMID: 25409854
- PMCID: PMC4245413
- DOI: 10.1007/s12105-014-0590-0
Fibro-osseous lesions of the craniofacial skeleton: an update
Abstract
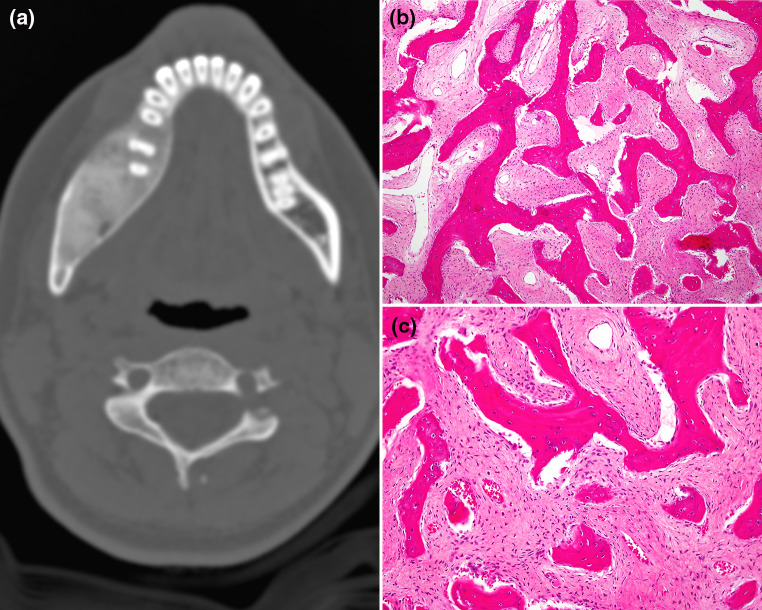
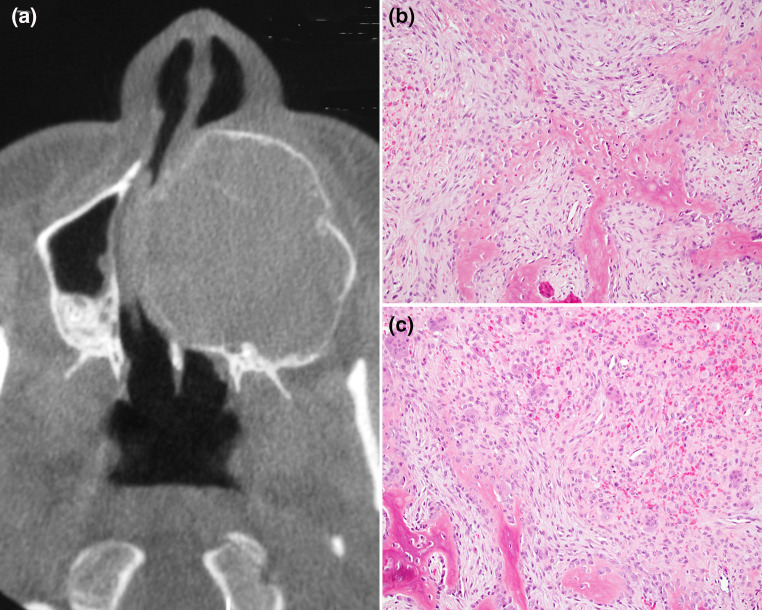
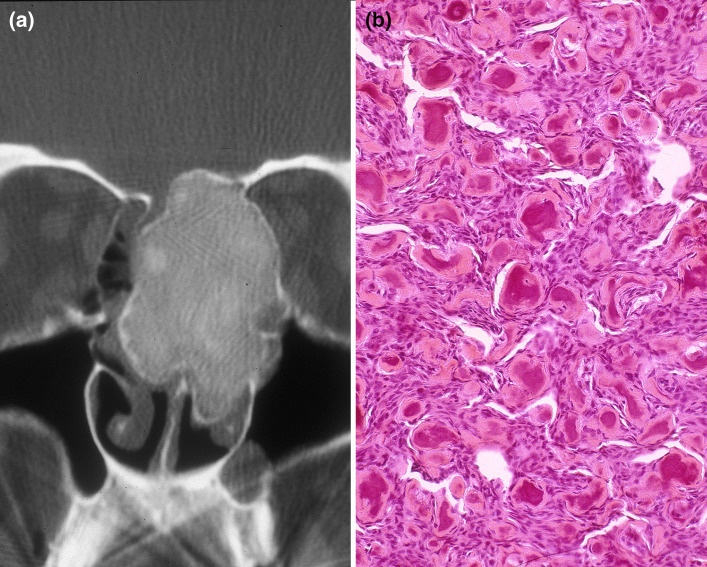
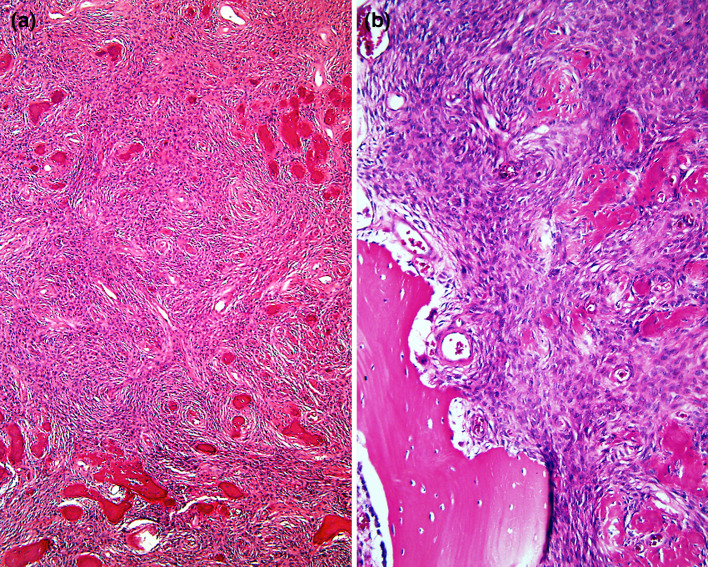
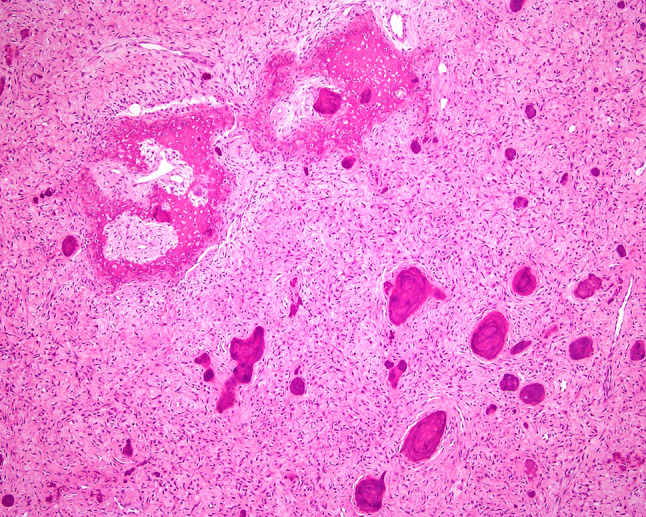
Benign fibro-osseous lesions of the craniofacial skeleton (BFOL) are a variant group of intraosseous disease processes that share similar microscopic features characterized by hypercellular fibroblastic stroma containing various combinations of bone or cementum-like tissue and other calcified structures [1-6]. Whereas some are diagnosable histologically, most require a combined assessment of clinical, microscopic and radiologic features. Some BFOL of the craniofacial complex are unique to that location whereas others are encountered in bones from other regions. Reactive, neoplastic, developmental and dysplastic pathologic processes are included under the rubric of BFOL and treatment varies from disease to disease. This review will discuss the clinical, microscopic and radiologic aspects of the more important types of BFOL of the craniofacial complex with updated information on underlying genetic and molecular pathogenic mechanisms of disease. Four main groups of BFOLs will be addressed.
Figures




References
-
- Hamner JE III, Scofield HH, Cornyn J (1968) Benign fibro-osseous lesions of periodontal membrane origin. An analysis of 249 cases. Cancer. 1968;22:861–78. - PubMed
-
- El-Mofty S. Bone lesions. In: Gnepp D, editor. Diagnostic surgical pathology of the head and neck, 2nd ed. Philadelphia: Saunders, Elsevier; 2009. p. 729–84.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
