

Metastatic tumors to the jaws and mouth
- PMID: 25409855
- PMCID: PMC4245411
- DOI: 10.1007/s12105-014-0591-z
Metastatic tumors to the jaws and mouth
Abstract
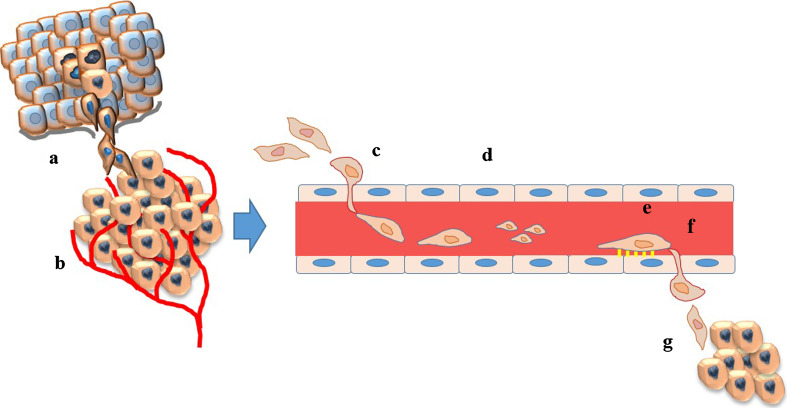
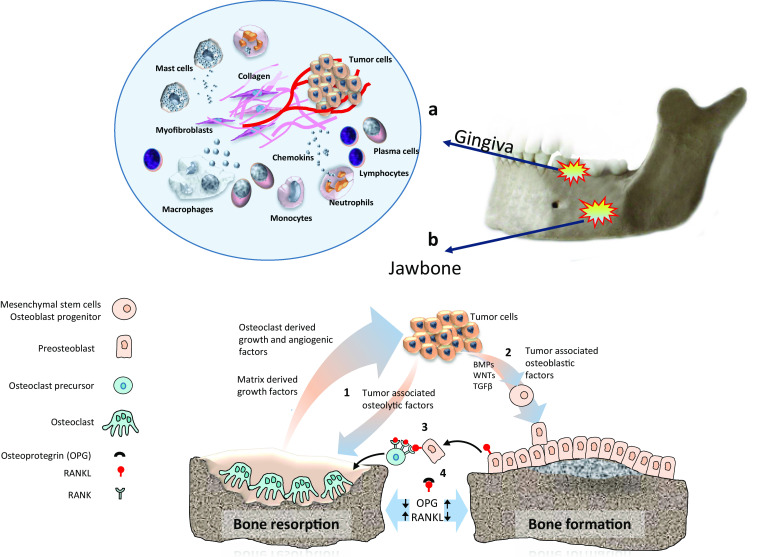
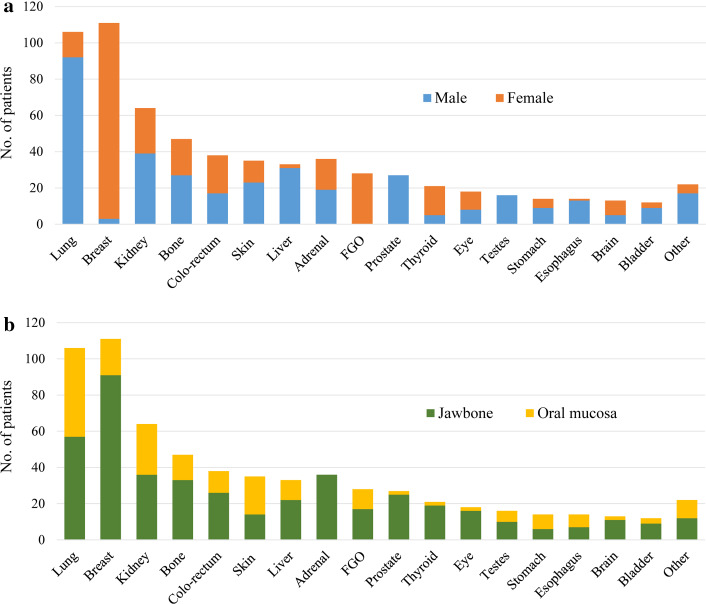
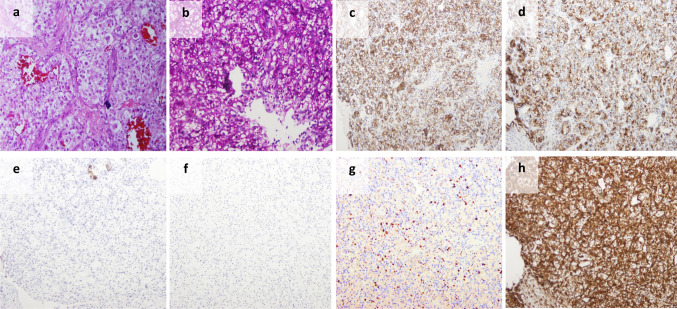
Metastatic dissemination to the oral cavity is rare and is usually the evidence of a wide spread disease with an average survival rate of 7 months. In almost a quarter of the cases, oral metastasis was found to be the first indication of an occult malignancy at a distant site. Metastatic lesions can be found anywhere in the oral cavity, however, the jaw bones with the molar area is the most frequently involved site. In the oral soft tissues, the gingiva is the most common site, suggesting the possible role of inflammation in the attraction of metastatic deposits. The most common primary malignancies presenting oral metastases were the lung, kidney, liver, and prostate for men, and breast, female genital organs, kidney, and colo-rectum for women. Most patients with jawbone metastasis complain of swelling, pain, and paresthesia. An exophytic lesion is the most common clinical presentation of metastatic lesions in the oral soft tissues. Early lesions, mainly those located in the gingiva, may resemble a hyperplastic or reactive lesion. Once a lesion is recognized as metastasis, the primary tumor site should be identified following clinical, radiological and histopathological investigations. If standardized diagnostic workup fails to detect the site of origin, then the term carcinoma of unknown primary is applied. Personalized medicine tools such as tissue-of-origin assays should be applied, either by immunohistochemical testing or by molecular-profiling methods as these may lead to a more favorable outcome.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
