

Cost-effectiveness of high, moderate and low-dose statins in the prevention of vascular events in the Brazilian public health system
- PMID: 25409878
- PMCID: PMC4387609
- DOI: 10.5935/abc.20140173
Cost-effectiveness of high, moderate and low-dose statins in the prevention of vascular events in the Brazilian public health system
Erratum in
-
Correction: Custo-efetividade de Estatinas em Dose Alta, Moderada e Baixa na Prevenção de Eventos Vasculares no SUS.Arq Bras Cardiol. 2015 Oct;105(4):445. doi: 10.5935/abc.20150138. Arq Bras Cardiol. 2015. PMID: 26559994 Free PMC article. No abstract available.
Abstract
Background: Statins have proven efficacy in the reduction of cardiovascular events, but the financial impact of its widespread use can be substantial.
Objective: To conduct a cost-effectiveness analysis of three statin dosing schemes in the Brazilian Unified National Health System (SUS) perspective.
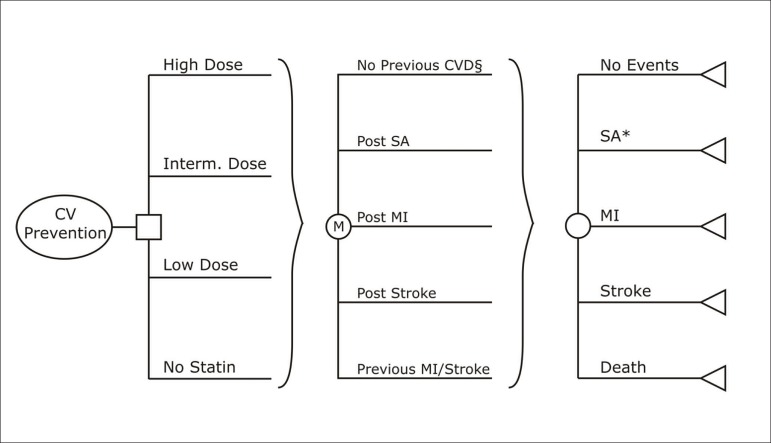
Methods: We developed a Markov model to evaluate the incremental cost-effectiveness ratios (ICERs) of low, intermediate and high intensity dose regimens in secondary and four primary scenarios (5%, 10%, 15% and 20% ten-year risk) of prevention of cardiovascular events. Regimens with expected low-density lipoprotein cholesterol reduction below 30% (e.g. simvastatin 10mg) were considered as low dose; between 30-40%, (atorvastatin 10mg, simvastatin 40 mg), intermediate dose; and above 40% (atorvastatin 20-80 mg, rosuvastatin 20mg), high-dose statins. Effectiveness data were obtained from a systematic review with 136,000 patients. National data were used to estimate utilities and costs (expressed as International Dollars - Int$). A willingness-to-pay (WTP) threshold equal to the Brazilian gross domestic product per capita (circa Int$11,770) was applied.
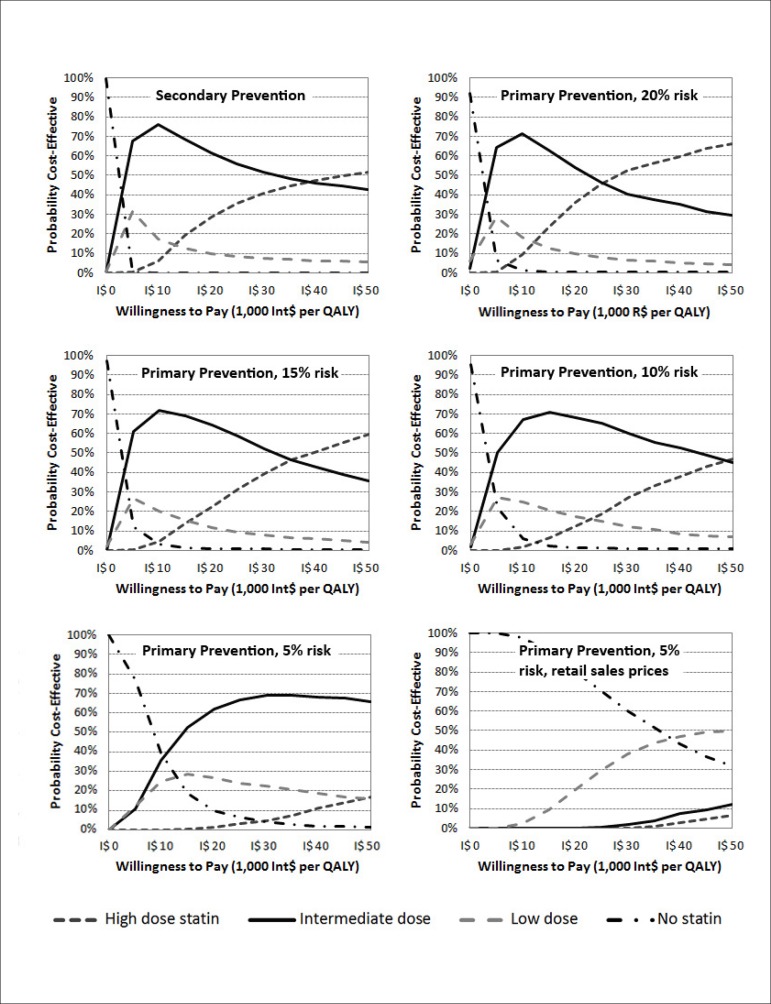
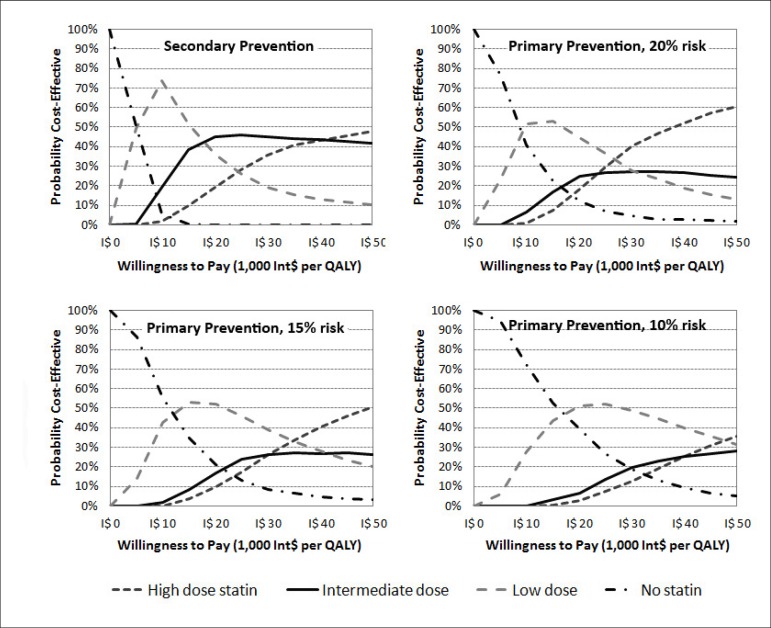
Results: Low dose was dominated by extension in the primary prevention scenarios. In the five scenarios, the ICER of intermediate dose was below Int$10,000 per QALY. The ICER of the high versus intermediate dose comparison was above Int$27,000 per QALY in all scenarios. In the cost-effectiveness acceptability curves, intermediate dose had a probability above 50% of being cost-effective with ICERs between Int$ 9,000-20,000 per QALY in all scenarios.
Conclusions: Considering a reasonable WTP threshold, intermediate dose statin therapy is economically attractive, and should be a priority intervention in prevention of cardiovascular events in Brazil.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Ward S, Lloyd Jones M, Pandor A, Holmes M, Ara R, Ryan A, et al. A systematic review and economic evaluation of statins for the prevention of coronary events. Health Technol Assess. 2007;11(14):1–160. - PubMed
-
- Mills EJ, Wu P, Chong G, Ghement I, Singh S, Akl EA, et al. Efficacy and safety of statin treatment for cardiovascular disease: a network meta-analysis of 170 255 patients from 76 randomized trials. QJM. 2011;104(2):109–124. - PubMed
-
- Estatinas na prevenção primária de eventos cardiovasculares. Boletim Brasileiro de Avaliação de Tecnologias em Saúde (BRATS) 2009;4(9):1–13.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
