

Biofortified orange maize is as efficacious as a vitamin A supplement in Zambian children even in the presence of high liver reserves of vitamin A: a community-based, randomized placebo-controlled trial
- PMID: 25411289
- PMCID: PMC4232019
- DOI: 10.3945/ajcn.114.087379
Biofortified orange maize is as efficacious as a vitamin A supplement in Zambian children even in the presence of high liver reserves of vitamin A: a community-based, randomized placebo-controlled trial
Abstract
Background: Biofortification is a strategy to relieve vitamin A (VA) deficiency. Biofortified maize contains enhanced provitamin A concentrations and has been bioefficacious in animal and small human studies.
Objective: The study sought to determine changes in total body reserves (TBRs) of vitamin A with consumption of biofortified maize.
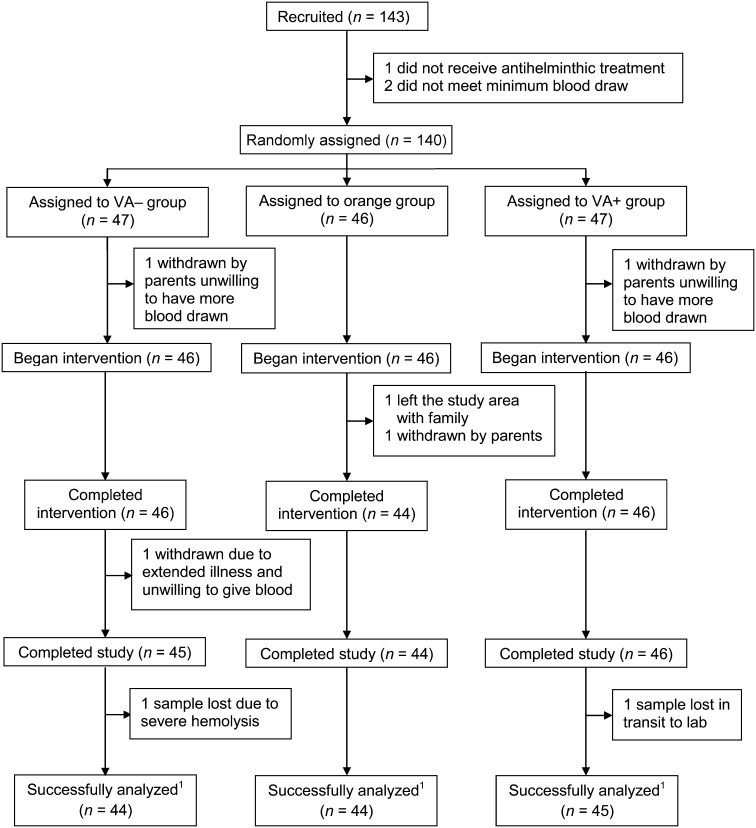
Design: A randomized, placebo-controlled biofortified maize efficacy trial was conducted in 140 rural Zambian children. The paired (13)C-retinol isotope dilution test, a sensitive biomarker for VA status, was used to measure TBRs before and after a 90-d intervention. Treatments were white maize with placebo oil (VA-), orange maize with placebo (orange), and white maize with VA in oil [400 μg retinol activity equivalents (RAEs) in 214 μL daily] (VA+).
Results: In total, 133 children completed the trial and were analyzed for TBRs (n = 44 or 45/group). Change in TBR residuals were not normally distributed (P < 0.0001); median changes (95% CI) were as follows: VA-, 13 (-19, 44) μmol; orange, 84 (21, 146) μmol; and VA+, 98 (24, 171) μmol. Nonparametric analysis showed no statistical difference between VA+ and orange (P = 0.34); both were higher than VA- (P = 0.0034). Median (95% CI) calculated liver reserves at baseline were 1.04 (0.97, 1.12) μmol/g liver, with 59% >1 μmol/g, the subtoxicity cutoff; none were <0.1 μmol/g, the deficiency cutoff. The calculated bioconversion factor was 10.4 μg β-carotene equivalents/1 μg retinol by using the middle 3 quintiles of change in TBRs from each group. Serum retinol did not change in response to intervention (P = 0.16) but was reduced with elevated C-reactive protein (P = 0.0029) and α-1-acid glycoprotein (P = 0.0023) at baseline.
Conclusions: β-Carotene from maize was efficacious when consumed as a staple food in this population and could avoid the potential for hypervitaminosis A that was observed with the use of preformed VA from supplementation and fortification. Use of more sensitive methods other than serum retinol alone, such as isotope dilution, is required to accurately assess VA status, evaluate interventions, and investigate the interaction of VA status and infection. This trial was registered at clinicaltrials.gov as NCT01814891.
Keywords: 13C-retinol dilution; Zambia; biofortified maize; plant carotenoids; retinol.
© 2014 American Society for Nutrition.
Figures


Comment in
-
Uncertainties of assessing total body vitamin A stores in community settings in low-income countries using the stable-isotope dilution methodology.Am J Clin Nutr. 2015 Aug;102(2):520-1. doi: 10.3945/ajcn.115.110825. Am J Clin Nutr. 2015. PMID: 26240192 Free PMC article. No abstract available.
-
Reply to G Lietz et al.Am J Clin Nutr. 2015 Aug;102(2):521-2. doi: 10.3945/ajcn.115.110973. Am J Clin Nutr. 2015. PMID: 26240193 Free PMC article. No abstract available.
References
-
- WHO. Global prevalence of vitamin A deficiency in populations at risk 1995–2005. WHO Global Database on Vitamin A Deficiency. Geneva (Switzerland): World Health Organization; 2009.
-
- Vitamin A supplementation coverage rate (% of children ages 6–59 months): World Development Indicators [Internet]. Washington, DC: The World Bank [cited 2014 May 10]. Available from: http://data.worldbank.org/indicator/SN.ITK.VITA.ZS.
-
- Fiedler JL, Lividini K, Kabaghe G, Zulu R, Tehinse J, Bermudez O, Jallier V, Guyondet C. Assessing Zambia's industrial fortification options: getting beyond changes in prevalence and cost-effectiveness. Food Nutr Bull 2013;34:501–19. - PubMed
-
- Kafwembe EM. The vitamin A status of Zambian children in a community of vitamin A supplementation and sugar fortification strategies as measured by the modified relative dose response (MRDR) test. Int J Vitam Nutr Res 2009;79:40–7. - PubMed
-
- Clewes C, Kankasa C. Report of the National Survey to evaluate the impact of vitamin A interventions in Zambia in July and November 2003 [Internet]. Lusaka (Zambia); National Food and Nutrition Commission of Zambia. 2003 [cited 2013 Dec 12]. Available from: http://www.micronutrient.org/nutritiontoolkit/ModuleFolders/12.Data_entr....
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
