

Pentraxin3 in chronic thromboembolic pulmonary hypertension: a new biomarker for screening from remitted pulmonary thromboembolism
- PMID: 25412085
- PMCID: PMC4239022
- DOI: 10.1371/journal.pone.0113086
Pentraxin3 in chronic thromboembolic pulmonary hypertension: a new biomarker for screening from remitted pulmonary thromboembolism
Abstract
Background: Pentraxin3 (PTX3) is a protein, which has multifaceted effects on innate immunity, angiogenesis, and vascular remodeling then could be a disease marker of acute myocardial infarction, heart failure, vasculitis. In addition, PTX3 has been recognized as a biomarker for pulmonary arterial hypertension, however whether it is the case in chronic thromboembolic pulmonary hypertension (CTEPH) remains unclear. Therefore, we investigated whether PTX3 would be a useful biomarker for detecting CTEPH with respect to differentiation from stable pulmonary thromboembolism (PTE), in comparison to other biomarkers.
Methods: Plasma PTX3 and brain natriuretic peptide (BNP) levels were measured in 70 patients with CTEPH at their first diagnostic right heart catheterization (CTEPH group) and in 20 patients with clinically stable PTE more than three months after the acute episode (control group). The levels of plasma C-reactive protein (CRP) and heart-type fatty acid-binding protein (H-FABP) were also analyzed to compare the diagnostic ability of these biomarkers.
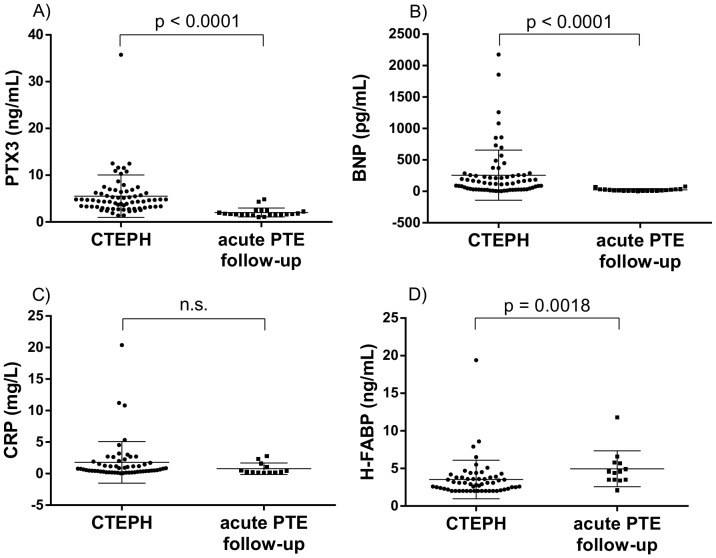
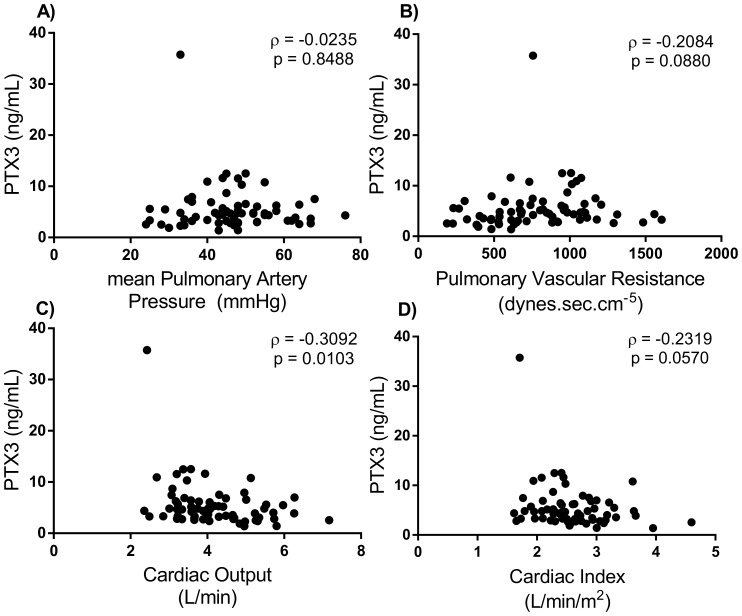
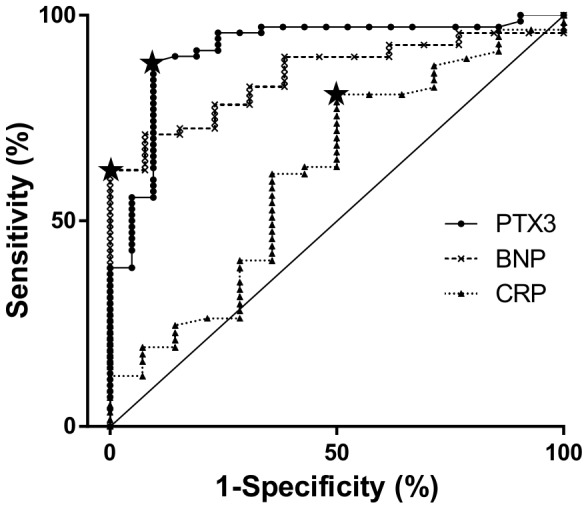
Results: The mean level of PTX3 (ng/mL) was significantly higher in the CTEPH group than in the control group (5.51±4.53 versus 2.01±0.96, respectively), and PTX3 levels had mild negative correlation with cardiac output. BNP levels were also higher in the CTEPH group and better correlated with pulmonary hemodynamics than PTX3. However, a receiver operating characteristic (ROC) curve showed PTX3 levels were better for detecting CTEPH, and could detect CTEPH patients with less severe pulmonary hemodynamics and low plasma BNP levels. There was no significant increase in CRP and H-FABP levels in the CTEPH patients.
Conclusions: Plasma PTX3 level was the most sensitive biomarker of CTEPH. Although plasma PTX3 levels did not correlate with the severity of the pulmonary hemodynamics compared to BNP, high levels in clinically stable patients following PTE should prompt a further work-up for CTEPH, which may lead to an early diagnosis.
Conflict of interest statement
Figures
Similar articles
-
Diagnostic values of serum BNP, PTX3, and VEGF in acute pulmonary embolism complicated by pulmonary artery hypertension and their correlations with severity of pulmonary artery hypertension.Immun Inflamm Dis. 2023 Sep;11(9):e986. doi: 10.1002/iid3.986. Immun Inflamm Dis. 2023. PMID: 37773724 Free PMC article.
-
Human pentraxin 3 (PTX3) as a novel biomarker for the diagnosis of pulmonary arterial hypertension.PLoS One. 2012;7(9):e45834. doi: 10.1371/journal.pone.0045834. Epub 2012 Sep 21. PLoS One. 2012. PMID: 23029266 Free PMC article.
-
Brain natriuretic peptide as noninvasive marker of the severity of right ventricular dysfunction in chronic thromboembolic pulmonary hypertension.Ann Thorac Surg. 2007 Aug;84(2):537-43. doi: 10.1016/j.athoracsur.2007.04.006. Ann Thorac Surg. 2007. PMID: 17643631
-
Pulmonary endarterectomy: part I. Pathophysiology, clinical manifestations, and diagnostic evaluation of chronic thromboembolic pulmonary hypertension.Semin Cardiothorac Vasc Anesth. 2014 Dec;18(4):319-30. doi: 10.1177/1089253214536621. Epub 2014 Jun 22. Semin Cardiothorac Vasc Anesth. 2014. PMID: 24958718 Review.
-
Chronic thromboembolic pulmonary hypertension: an underdiagnosed entity?Hosp Pract (1995). 2012 Aug;40(3):71-9. doi: 10.3810/hp.2012.08.991. Hosp Pract (1995). 2012. PMID: 23086096 Review.
Cited by
-
Diagnostic advances and opportunities in chronic thromboembolic pulmonary hypertension.Eur Respir Rev. 2015 Jun;24(136):253-62. doi: 10.1183/16000617.00000915. Eur Respir Rev. 2015. PMID: 26028637 Free PMC article. Review.
-
Expression and influence of pentraxin-3, HbAlc and ApoA1/ApoB in serum of patients with acute myocardial infarction combined with diabetes mellitus type 2.Exp Ther Med. 2018 May;15(5):4395-4399. doi: 10.3892/etm.2018.5930. Epub 2018 Mar 6. Exp Ther Med. 2018. PMID: 29731826 Free PMC article.
-
Increased serum pentraxin-3 level predicts poor prognosis in patients with colorectal cancer after curative surgery, a cohort study.Medicine (Baltimore). 2018 Oct;97(40):e11780. doi: 10.1097/MD.0000000000011780. Medicine (Baltimore). 2018. PMID: 30290589 Free PMC article.
-
Circulating biomarkers in chronic thromboembolic pulmonary hypertension.Pulm Circ. 2019 Apr-Jun;9(2):2045894019844480. doi: 10.1177/2045894019844480. Pulm Circ. 2019. PMID: 30942132 Free PMC article.
-
The inflammatory protein Pentraxin 3 in cardiovascular disease.Immun Ageing. 2016 Aug 24;13(1):25. doi: 10.1186/s12979-016-0080-1. eCollection 2016. Immun Ageing. 2016. PMID: 27559355 Free PMC article. Review.
References
-
- Lang IM, Pesavento R, Bonderman D, Yuan JX (2013) Risk factors and basic mechanisms of chronic thromboembolic pulmonary hypertension: a current understanding. Eur Respir J 41: 462–468. - PubMed
-
- Mayer E, Jenkins D, Lindner J, D'Armini A, Kloek J, et al. (2011) Surgical management and outcome of patients with chronic thromboembolic pulmonary hypertension: results from an international prospective registry. J Thorac Cardiovasc Surg 141: 702–710. - PubMed
-
- Kim NH (2006) Assessment of operability in chronic thromboembolic pulmonary hypertension. Proc Am Thorac Soc 3: 584–588. - PubMed
-
- Pepke-Zaba J, Delcroix M, Lang I, Mayer E, Jansa P, et al. (2011) Chronic thromboembolic pulmonary hypertension (CTEPH): results from an international prospective registry. Circulation 124: 1973–1981. - PubMed
-
- Kim NH, Delcroix M, Jenkins DP, Channick R, Dartevelle P, et al. (2013) Chronic thromboembolic pulmonary hypertension. J Am Coll Cardiol 62: D92–99. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
