

Review
doi: 10.1038/eye.2014.262.
Epub 2014 Nov 21.
A brief review of the clinical anatomy of the vestibular-ocular connections-how much do we know?
Affiliations
- PMID: 25412719
- PMCID: PMC4330278
- DOI: 10.1038/eye.2014.262
Item in Clipboard
Review
A brief review of the clinical anatomy of the vestibular-ocular connections-how much do we know?
Eye (Lond).
2015 Feb.
Abstract
The basic connectivity from the vestibular labyrinth to the eye muscles (vestibular ocular reflex, VOR) has been elucidated in the past decade, and we summarise this in graphic format. We also review the concept of 'velocity storage', a brainstem integrator that prolongs vestibular responses. Finally, we present new discoveries of how complex visual stimuli, such as binocular rivalry, influence VOR processing. In contrast to the basic brainstem circuits, cortical vestibular circuits are far from being understood, but parietal-vestibular nuclei projections are likely to be involved.
Figures
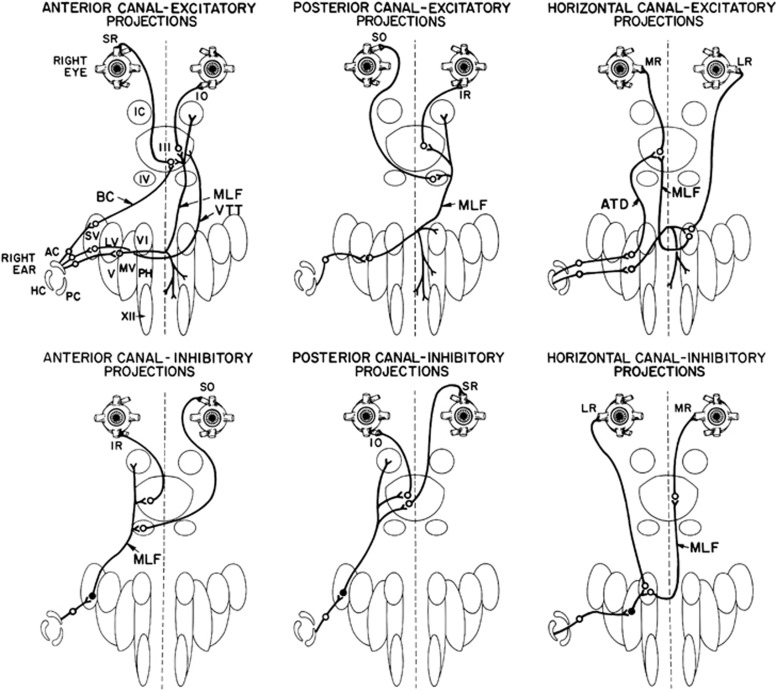
Summary of the direct connections of the semicircular canals to the oculomotor neurons and muscles (from Leigh and Zee with permission). Each canal has excitatory projections (open circles) to the acting motoneurons and inhibitory projections (filled up circles) to the antagonistic motoneurons. Abbreviations: AC/PC/HC, anterior/posterior/horizontal canal; SR/MR/IR/LR, superior/medial/inferior/lateral rectus; SO/IO, superior/inferior oblique; III/IV/VI, third/fourth/sixth cranial nerve nucleus; IC, interstitial nucleus of Cajal; VTT, ventral tegmental tract; MLF, medial longitudinal fasciculus; ATD, ascending tract of Deiters; SV/LV/MV/V, superior/lateral/medial/inferior vestibular nucleus; BC, brachium conjunctivum; XII, hypoglossal nucleus; PH, prepositus hypoglossal nucleus.
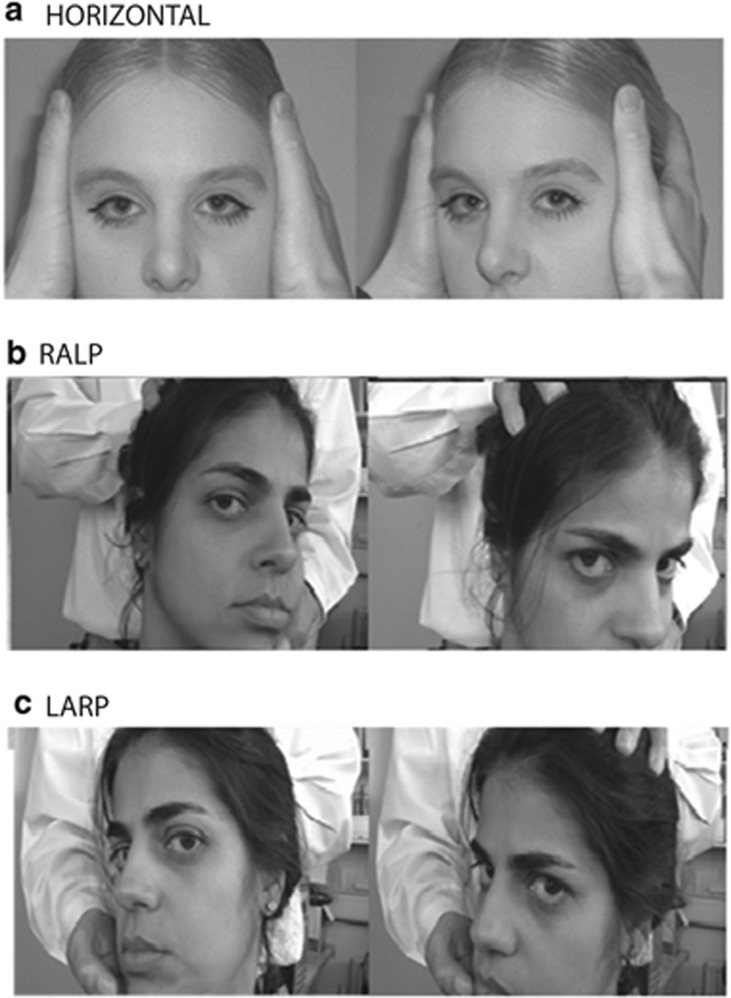
The HIT. (a). (Top picture) the clinician instructs the patient to fixate a target straight ahead and then turns the head rapidly either to the left or right. A right head turn as shown tests the right horizontal canal. The normal response results in a slow-phase compensatory eye movement to the left, which occurs almost instantaneously (modified from, Bronstein and Lampert with permission). In (b) (middle picture), the clinician turns the patients head to the left by ∼30°, to align the right anterior and left posterior (RALP) semicircular canals along a vertical axis. The clinician then places one hand on the top of the patient's head and one hand below and rapidly thrusts the head either forwards (testing right anterior canal) or backwards (testing left posterior canal). In (c) (bottom picture), the clinician asks the patient to turn their head to the right by ∼30°, to align the left anterior and right posterior (LARP) semicircular canals along a vertical axis. The clinician then places one hand on top of the patient's head and one hand below and rapidly thrusts the head either forwards (testing left anterior canal) or backwards (testing right posterior canal).
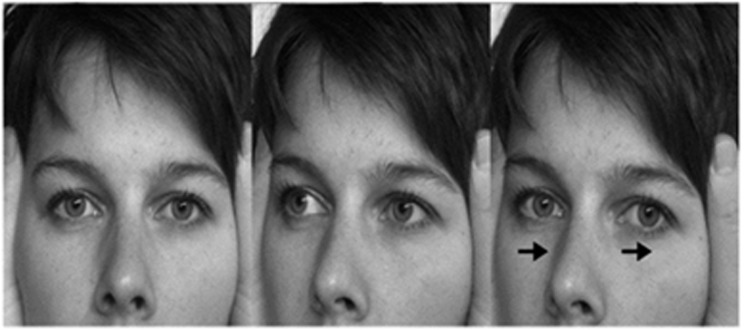
Head impulse test of the right horizontal canal in a simulated patient with loss of vestibular function on the right. Here, the eyes first move in the direction of the head turn (owing to absent VOR) before a corrective refixating saccade occurs in the opposite direction (from Bronstein and Lempert with permission).
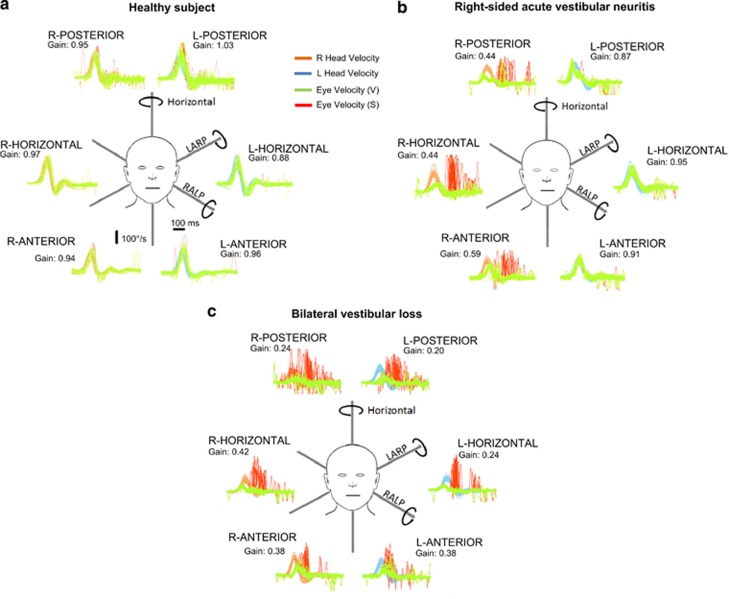
The plots represent time series showing superimposed recordings of the head velocity stimulus (brown for right canals and blue for left canals) and the slow-phase eye-velocity responses (eye velocity VOR—green traces) to 20 randomised (either direction) head turns, to sequentially test all the semicircular canals in turn in (a) a healthy subject, (b) a patient with right-sided acute vestibular neuritis and (c) a patient with bilateral vestibular loss. Overt or covert saccades are shown as red traces, and can be seen when testing the side of the lesion in the vestibular neuritis patient (ie, right) and when testing both the right and left sides of the patient with bilateral vestibular failure. Note that in this figure the eye velocity has been inverted to allow for a comparison with head velocity, and for illustration purposes only both leftward and rightward head movements are shown as positive. The average VOR gain value (eye velocity/head velocity) is shown next to each response.
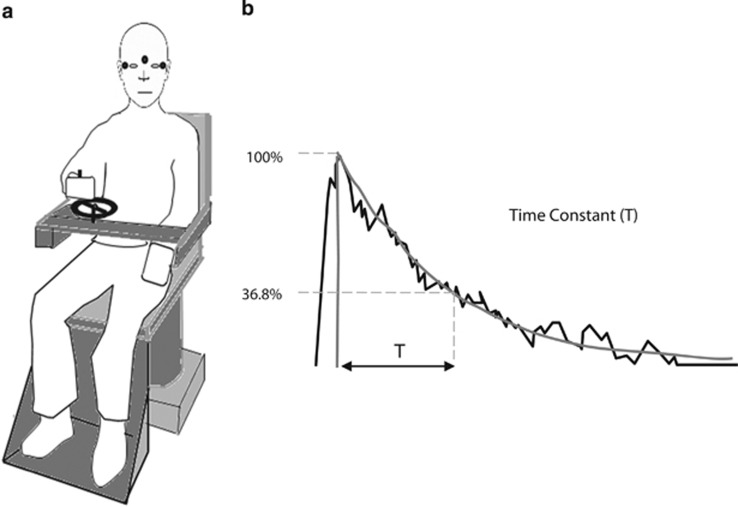
Diagrammatic representation of the vestibular perception test. (a) Subject is shown holding the handle of a tachometer wheel, which the subject is instructed to turn as to indicate their subjective perception of the rotational stimuli during 90°/s chair rotation either to the right or left. EOG electrodes seen in the figure by small black circles simultaneously capture nystagmus thus allowing us to compare vestibulo-ocular and vestibulo-perceptual responses. Subjects are instructed to turn the wheel as fast as possible initially on chair acceleration or deceleration for the first couple of seconds. From then on, the subject is asked to slow down the turning of the tachometer wheel gradually to match their own perceived turning sensation and eventually stop turning the wheel at the point that they no longer feel the rotation. (b) Tachometer output in a normal subject during a rotational stopping response. This output is fitted with an exponential curve and the time constant of decay is measured (typically between 15–18 s).
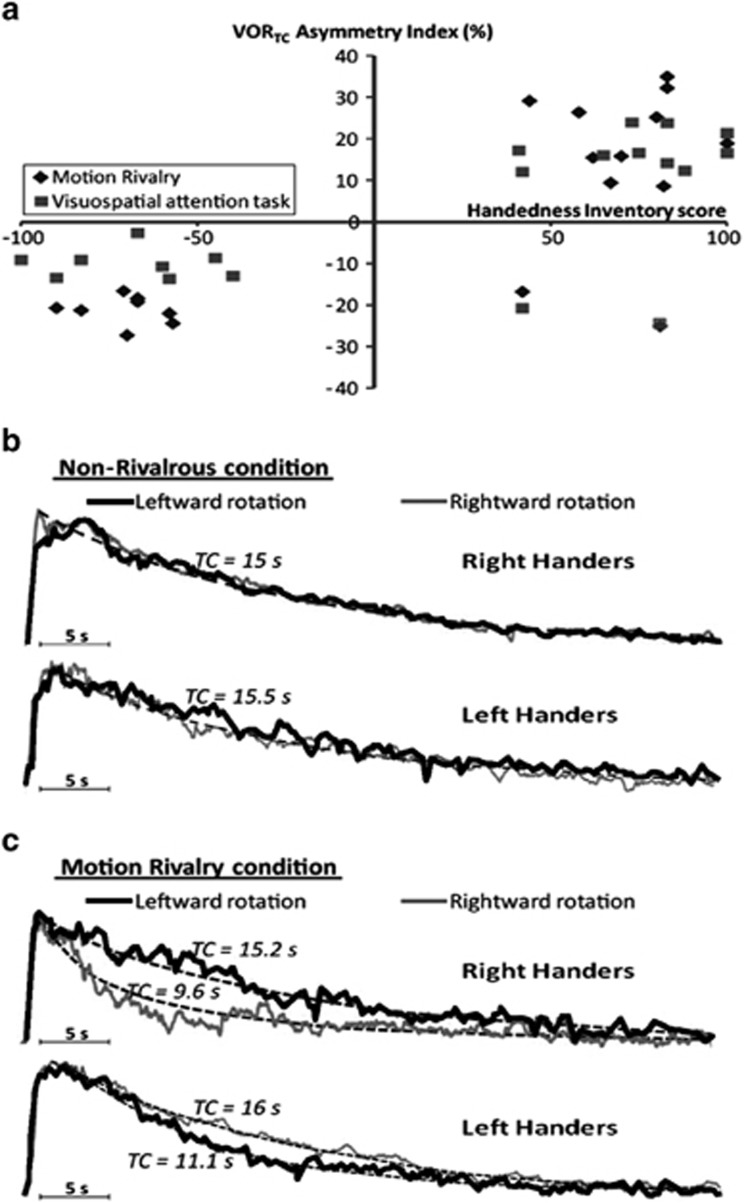
Shows a summary for results for the effects of binocular rivalry and the visuospatial working memory tasks upon the VOR. (a) Plots of each subject's individual asymmetry index (ie, degree of nystagmus suppression) and handedness inventory score. Right handers showed a positive asymmetry index except for two subjects who were retrained left handers in both the motion binocular rivalry condition (diamonds) and visuospatial task (squares). In contrast, all left-handed subjects and the two retrained right-handed subjects had a negative VORTC asymmetry index. (b and c) Plots of the exponential grand averages for the eye velocity for right- and left-handed subjects. (b) When a control visual stimulus was presented the VOR was symmetrical following either rightward or leftward rotations (overlapping black and grey curves). (c) The VOR following the viewing of motion rivalry is shown. Note that in right-handed subjects the VOR was supressed following rightward rotation (grey curve), whereas in left-handed subjects the VOR was supressed following leftward rotations (black curve).
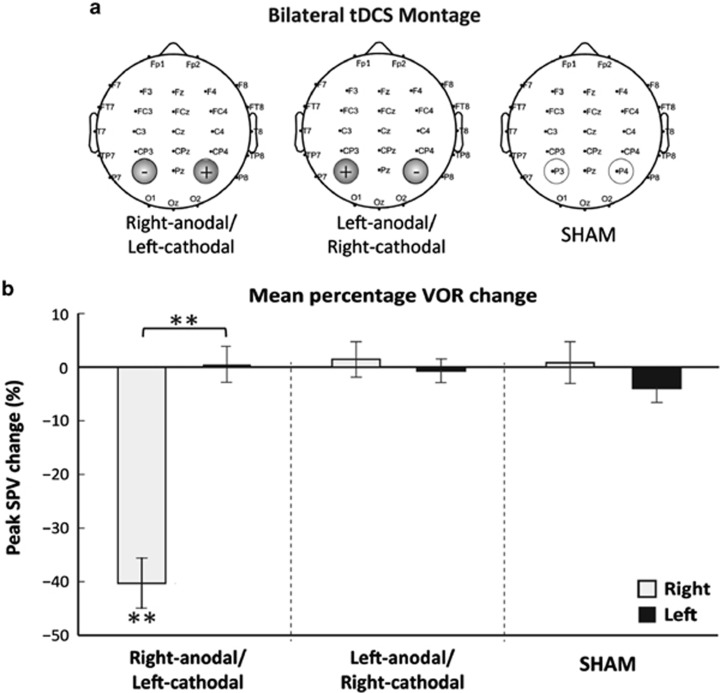
(a) tDCS montage used during bilateral stimulation. The electrodes were placed over the right (P4) and left (P3) parietal hemispheres respectively according to the 10–20 EEG international positioning system. Three types of bilateral parietal tDCS stimulation were applied: anodal stimulation over right hemisphere, cathodal stimulation over right hemisphere, and SHAM a control condition. (b) Right-anodal stimulation resulted in asymmetrical modulation of the VOR with a significant decrease in peak slow-phase velocity (SPV) during the right caloric with no change observed during the left caloric. Neither right-cathodal stimulation nor SHAM resulted in any VOR modulation of peak SPV. Data marked ** significant at P<0.001.
References
-
- Leigh JR, Zee DS.The Neurology of Eye Movements5th ednOxford University Press: New York; 2015
-
- Bronstein AM. Vision and vertigo: some visual aspects of vestibular disorders. J Neurol. 2004;251 (4:381–387. - PubMed
-
- Halmagyi GM, Curthoys IS. A clinical sign of canal paresis. Arch Neurol. 1988;45 (7:737–739. - PubMed
-
- Weber KP, MacDougall HG, Halmagyi GM, Curthoys IS. Impulsive testing of semicircular-canal function using video-oculography. Ann N Y Acad Sci. 2009;1164:486–491. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
