

Multimodality imaging of Alzheimer disease and other neurodegenerative dementias
- PMID: 25413136
- PMCID: PMC4702268
- DOI: 10.2967/jnumed.114.141416
Multimodality imaging of Alzheimer disease and other neurodegenerative dementias
Abstract
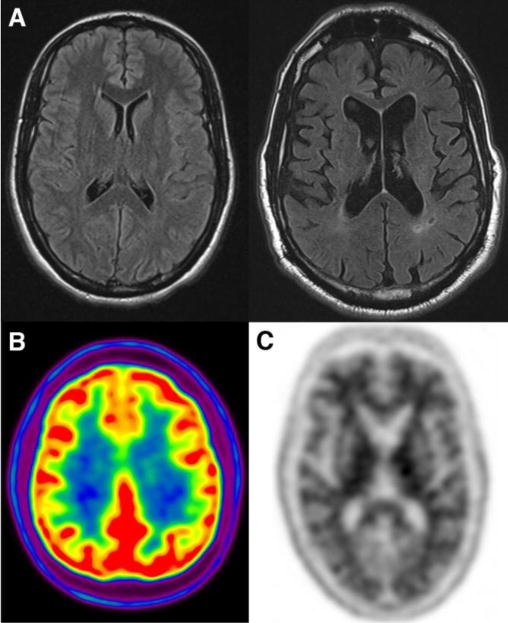
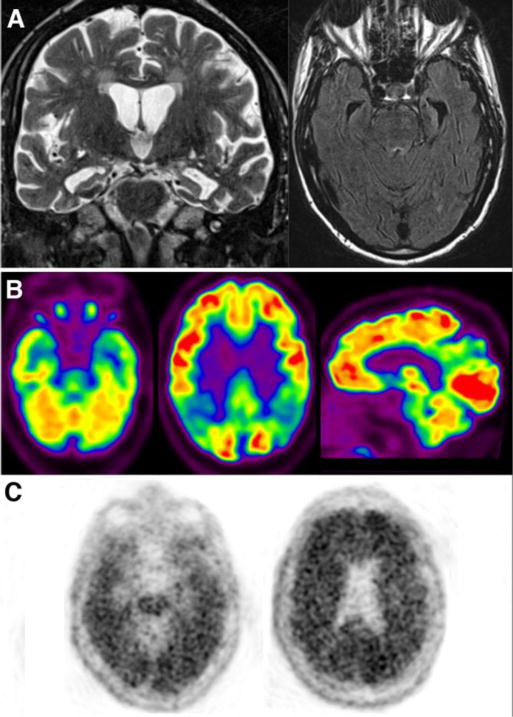
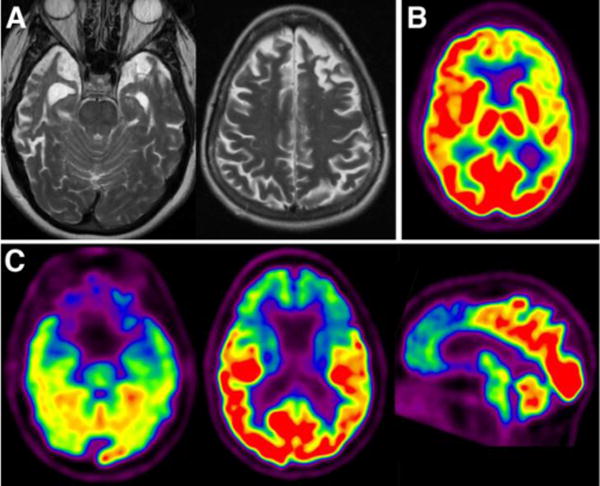
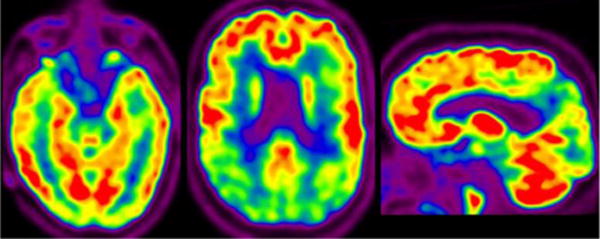
Neurodegenerative diseases, such as Alzheimer disease, result in cognitive decline and dementia and are a leading cause of mortality in the growing elderly population. These progressive diseases typically have an insidious onset, with overlapping clinical features early in the disease course that make diagnosis challenging. The neurodegenerative diseases are associated with characteristic, although not completely understood, changes in the brain: abnormal protein deposition, synaptic dysfunction, neuronal injury, and neuronal death. Neuroimaging biomarkers-principally regional atrophy on structural MR imaging, patterns of hypometabolism on (18)F-FDG PET, and detection of cerebral amyloid plaque on amyloid PET--are able to evaluate the patterns of these abnormalities in the brain to improve early diagnosis and help predict the disease course. These techniques have unique strengths and synergies in multimodality evaluation of the patient with cognitive decline or dementia. This review discusses the key imaging biomarkers from MR imaging, (18)F-FDG PET, and amyloid PET; the imaging features of the most common neurodegenerative dementias; the role of various neuroimaging studies in differential diagnosis and prognosis; and some promising imaging techniques under development.
Keywords: Alzheimer disease; FDG PET; MRI; amyloid PET; neurodegeneration.
© 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
Figures

References
-
- Fox C, Lafortune L, Boustani M, Dening T, Rait G, Brayne C. Screening for dementia–is it a no brainer? International journal of clinical practice. 2013;67:1076–1080. - PubMed
-
- World Alzheimer Report 2011. http://wwwalzcouk/research/world-report-2011.
-
- Josephs KA. Frontotemporal dementia and related disorders: deciphering the enigma. Annals of neurology. 2008;64:4–14. - PubMed
-
- Herholz K. Perfusion SPECT and FDG-PET. International psychogeriatrics/IPA. 2011;23(Suppl 2):S25–31. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical