

Preconception care: screening and management of chronic disease and promoting psychological health
- PMID: 25415675
- PMCID: PMC4196564
- DOI: 10.1186/1742-4755-11-S3-S5
Preconception care: screening and management of chronic disease and promoting psychological health
Abstract
Introduction: A large proportion of women around the world suffer from chronic diseases including mental health diseases. In the United States alone, over 12% of women of reproductive age suffer from a chronic medical condition, especially diabetes and hypertension. Chronic diseases significantly increase the odds for poor maternal and newborn outcomes in pregnant women.
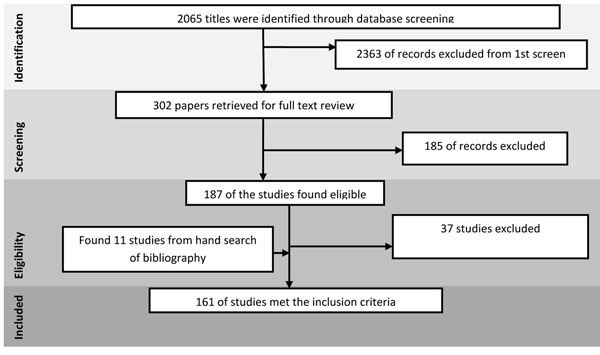
Methods: A systematic review and meta-analysis of the evidence was conducted to ascertain the possible impact of preconception care for preventing and managing chronic diseases and promoting psychological health on maternal, newborn and child health outcomes. A comprehensive strategy was used to search electronic reference libraries, and both observational and clinical controlled trials were included. Cross-referencing and a separate search strategy for each preconception risk and intervention ensured wider study capture.
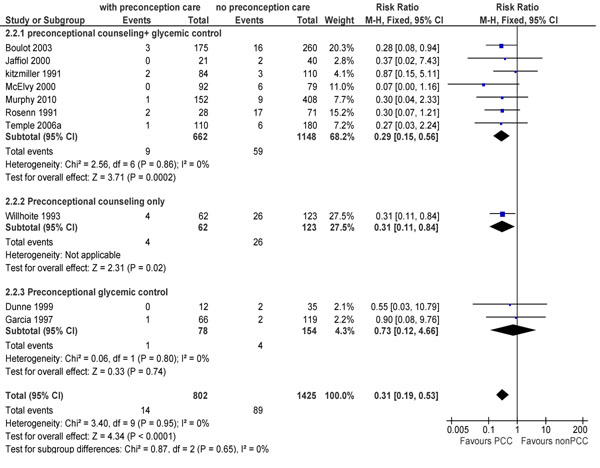
Results: Maternal prepregnancy diabetic care is a significant intervention that reduces the occurrence of congenital malformations by 70% (95% Confidence Interval (CI): 59-78%) and perinatal mortality by 69% (95% CI: 47-81%). Furthermore, preconception management of epilepsy and phenylketonuria are essential and can optimize maternal, fetal and neonatal outcomes if given before conception. Ideally changes in antiepileptic drug therapy should be made at least 6 months before planned conception. Interventions specifically targeting women of reproductive age suffering from a psychiatric condition show that group-counseling and interventions leading to empowerment of women have reported non-significant reduction in depression (economic skill building: Mean Difference (MD) -7.53; 95% CI: -17.24, 2.18; counseling: MD-2.92; 95% CI: -13.17, 7.33).
Conclusion: While prevention and management of the chronic diseases like diabetes and hypertension, through counseling, and other dietary and pharmacological intervention, is important, delivering solutions to prevent and respond to women's psychological health problems are urgently needed to combat this leading cause of morbidity.
Figures



References
-
- Kitzmiller JL, Buchanan TA, Kjos S, Combs CA, Ratner RE. Pre-conception care of diabetes, congenital malformations, and spontaneous abortions. Diabetes Care. 1996;19(5):514–541. - PubMed
-
- Ray JG, Vermeulen MJ, Meier C, Wyatt PR. Risk of congenital anomalies detected during antenatal serum screening in women with pregestational diabetes. Qjm. 2004;97(10):651. - PubMed
-
- Casey BM, Dashe JS, Wells CE, McIntire DD, Byrd W, Leveno KJ, Cunningham FG. Subclinical hypothyroidism and pregnancy outcomes. Obstetrics & Gynecology. 2005;105(2):239. - PubMed
-
- Koch R, Friedman E, Azen C, Hanley W, Levy H, Matalon R, Rouse B, Trefz F, Waisbren S, Michals-Matalon K. The international collaborative study of maternal phenylketonuria: status report 1998. European journal of pediatrics. 2000;159(14):156–160. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
