

Inflammatory markers and extent and progression of early atherosclerosis: Meta-analysis of individual-participant-data from 20 prospective studies of the PROG-IMT collaboration
- PMID: 25416041
- PMCID: PMC4544641
- DOI: 10.1177/2047487314560664
Inflammatory markers and extent and progression of early atherosclerosis: Meta-analysis of individual-participant-data from 20 prospective studies of the PROG-IMT collaboration
Abstract
Background: Large-scale epidemiological evidence on the role of inflammation in early atherosclerosis, assessed by carotid ultrasound, is lacking. We aimed to quantify cross-sectional and longitudinal associations of inflammatory markers with common-carotid-artery intima-media thickness (CCA-IMT) in the general population.
Methods: Information on high-sensitivity C-reactive protein, fibrinogen, leucocyte count and CCA-IMT was available in 20 prospective cohort studies of the PROG-IMT collaboration involving 49,097 participants free of pre-existing cardiovascular disease. Estimates of associations were calculated within each study and then combined using random-effects meta-analyses.
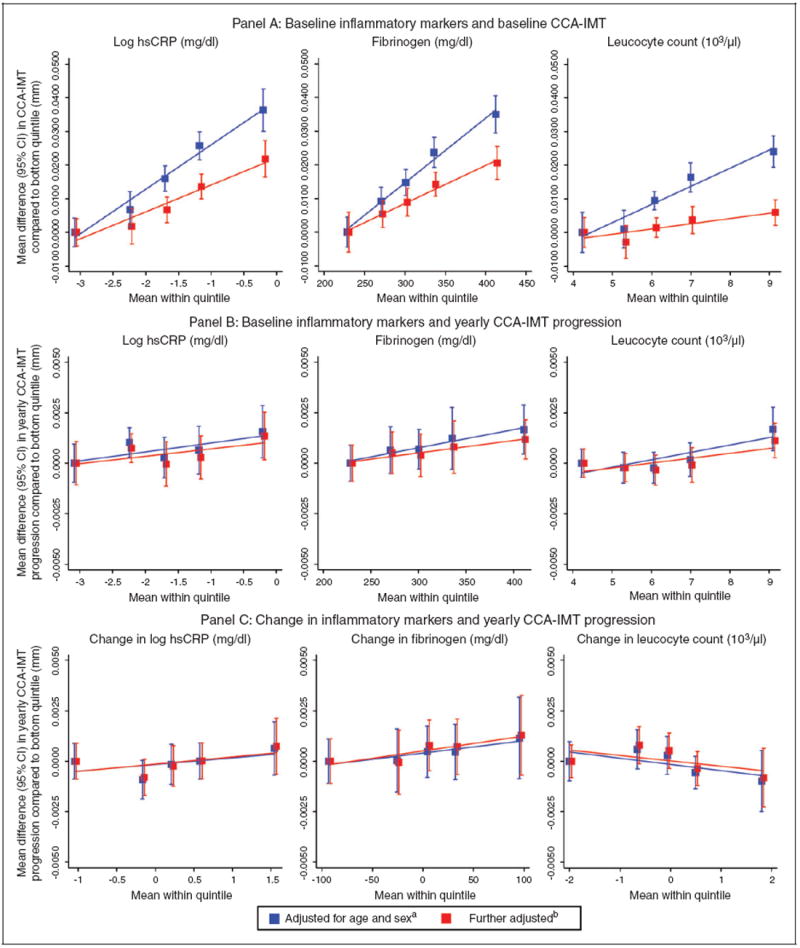
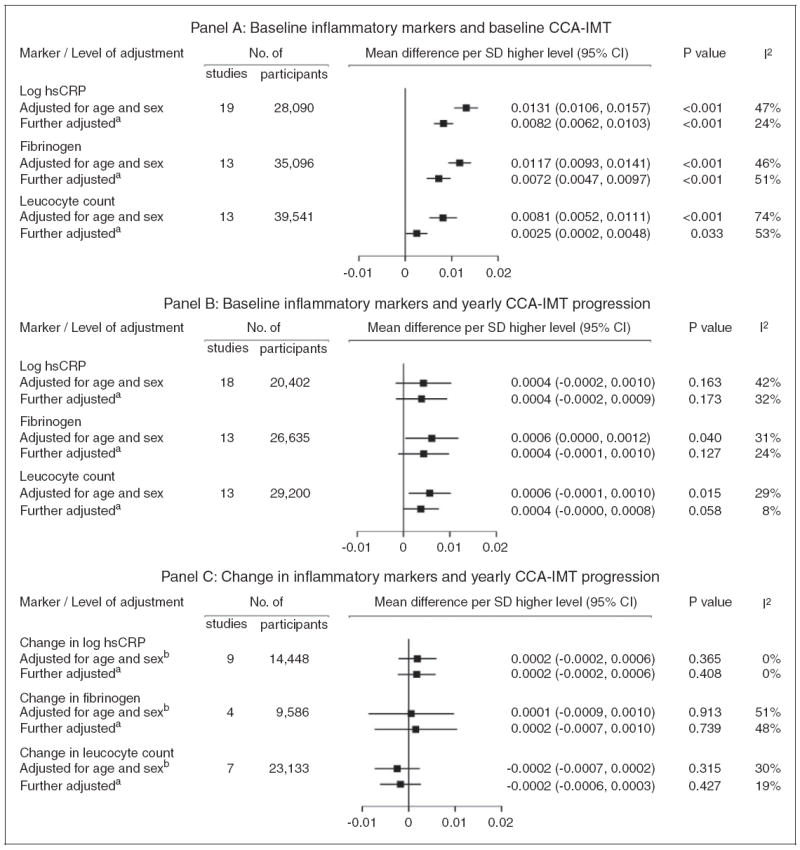
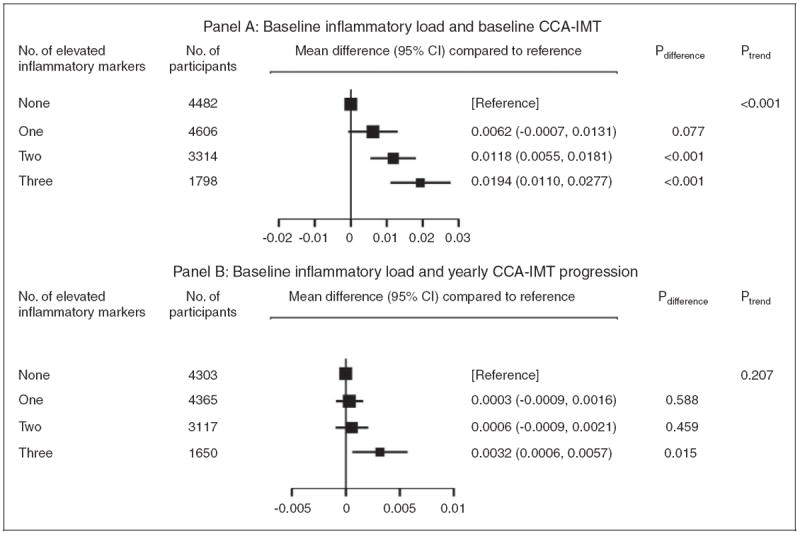
Results: Mean baseline CCA-IMT amounted to 0.74 mm (SD = 0.18) and mean CCA-IMT progression over a mean of 3.9 years to 0.011 mm/year (SD = 0.039). Cross-sectional analyses showed positive linear associations between inflammatory markers and baseline CCA-IMT. After adjustment for traditional cardiovascular risk factors, mean differences in baseline CCA-IMT per one-SD higher inflammatory marker were: 0.0082 mm for high-sensitivity C-reactive protein (p < 0.001); 0.0072 mm for fibrinogen (p < 0.001); and 0.0025 mm for leucocyte count (p = 0.033). 'Inflammatory load', defined as the number of elevated inflammatory markers (i.e. in upper two quintiles), showed a positive linear association with baseline CCA-IMT (p < 0.001). Longitudinal associations of baseline inflammatory markers and changes therein with CCA-IMT progression were null or at most weak. Participants with the highest 'inflammatory load' had a greater CCA-IMT progression (p = 0.015).
Conclusion: Inflammation was independently associated with CCA-IMT cross-sectionally. The lack of clear associations with CCA-IMT progression may be explained by imprecision in its assessment within a limited time period. Our findings for 'inflammatory load' suggest important combined effects of the three inflammatory markers on early atherosclerosis.
Keywords: Inflammation; atherosclerosis; meta-analysis.
© The European Society of Cardiology 2014.
Conflict of interest statement
SA has received speaker’s honoraria from Sanofi, Siemens, Pfizer, Boehringer-Ingelheim, Orion Pharma, and Astra Zeneza and is on the advisory board for Astra Zeneca. OHF works in ErasmusAGE, a centre for aging research across the life course funded by Nestlé Nutrition (Nestec Ltd), Metagenics Inc., and AXA. Nestlé Nutrition (Nestec Ltd.), Metagenics Inc. and AXA had no role in design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review or approval of the manuscript. MHO received a Research Grant from Merck & Co., Inc., West Point, PA. None of the other authors report conflicts of interest.
Figures
References
-
- Den Ruijter HM, Peters SAE, Anderson TJ, et al. Common carotid intima-media thickness measurements in cardiovascular risk prediction: A meta-analysis. JAMA. 2012;308:796–803. - PubMed
-
- Baldassarre D, Nyyssönen K, Rauramaa R, et al. Cross-sectional analysis of baseline data to identify the major determinants of carotid intima-media thickness in a European population: The IMPROVE study. Eur Heart J. 2010;31:614–622. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC085080/HL/NHLBI NIH HHS/United States
- N01HC85084/HC/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- R01 DE013094/DE/NIDCR NIH HHS/United States
- N01HC85085/HC/NHLBI NIH HHS/United States
- N01 HC085085/HC/NHLBI NIH HHS/United States
- R37 NS029993/NS/NINDS NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- R01 HL080295/HL/NHLBI NIH HHS/United States
- N01 HC085084/HC/NHLBI NIH HHS/United States
- HL080295/HL/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- N01 HC55222/HC/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- RG/08/014/24067/BHF_/British Heart Foundation/United Kingdom
- MR/L003120/1/MRC_/Medical Research Council/United Kingdom
- N01HC45133/HC/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- R37 NS 029993/NS/NINDS NIH HHS/United States
- N01HC35129/HC/NHLBI NIH HHS/United States
- N01 HC045133/HC/NHLBI NIH HHS/United States
- AG023629/AG/NIA NIH HHS/United States
- N01 HC035129/HC/NHLBI NIH HHS/United States
- R56 AG023629/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
