

Components of hemodynamic load and cardiovascular events: the Framingham Heart Study
- PMID: 25416177
- PMCID: PMC4308473
- DOI: 10.1161/CIRCULATIONAHA.114.011357
Components of hemodynamic load and cardiovascular events: the Framingham Heart Study
Abstract
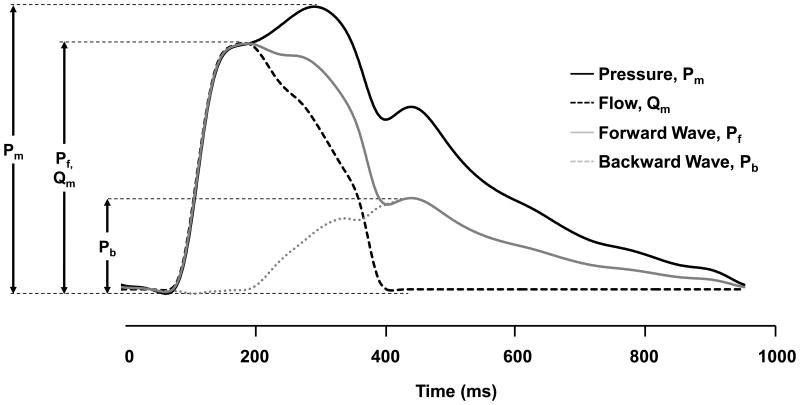
Background: Elevated blood pressure is the leading modifiable risk factor for cardiovascular disease (CVD) and premature death. The blood pressure waveform consists of discrete hemodynamic components, derived from measured central pressure and flow, which may contribute separately to risk for an adverse outcome. However, pressure-flow measures have not been studied in a large, community-based sample.
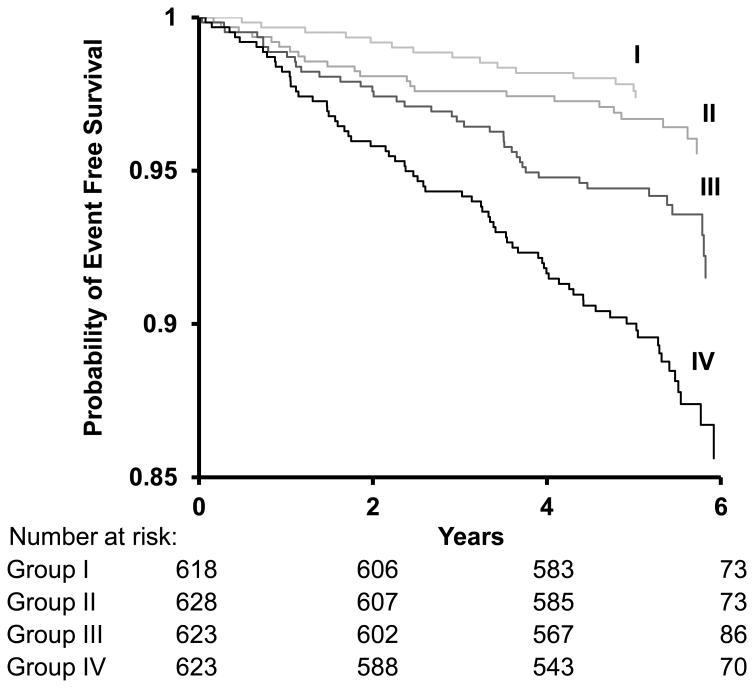
Methods and results: We used proportional hazards models to examine the association of incident CVD with forward pressure wave amplitude, mean arterial pressure, and global reflection coefficient derived from wave separation analysis and echocardiography in 2492 participants (mean age 66±9 years, 56% women) in the Framingham Heart Study. During follow-up (0.04-6.8 years), 149 participants (6%) had a CVD event. In multivariable models adjusting for age, sex, antihypertensive therapy, body mass index, heart rate, total and high-density lipoprotein cholesterol concentrations, smoking, and the presence of diabetes mellitus, forward pressure wave amplitude (hazard ratio, 1.40; 95% confidence interval, 1.16-1.67; P=0.0003) was associated with incident CVD, whereas mean arterial pressure (hazard ratio, 1.10; 95% confidence interval, 0.94-1.29; P=0.25) and global wave reflection (hazard ratio, 0.93; 95% confidence interval, 0.78-1.12; P=0.58) were not. After adding systolic blood pressure and carotid-femoral pulse wave velocity to the model, forward pressure wave amplitude persisted as a correlate of events (hazard ratio, 1.33; 95% confidence interval, 1.05-1.68; P=0.02).
Conclusions: Higher forward pressure wave amplitude (a measure of proximal aortic geometry and stiffness) was associated with increased risk for incident CVD, whereas mean arterial pressure and relative wave reflection (correlates of resistance vessel structure and function) were not associated with increased risk for incident CVD.
Keywords: cardiovascular diseases; hemodynamics; pulsatile flow.
© 2014 American Heart Association, Inc.
Conflict of interest statement
Figures
References
-
- Fields LE, Burt VL, Cutler JA, Hughes J, Roccella EJ, Sorlie P. The burden of adult hypertension in the United States 1999 to 2000: a rising tide. Hypertension. 2004;44:398–404. - PubMed
-
- Lawes CMM, Vander Hoorn S, Rodgers A. Global burden of blood-pressure-related disease, 2001. Lancet. 2008;371:1513–1518. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, Jones DW, Materson BJ, Oparil S, Wright JT, Jr, Roccella EJ National High Blood Pressure Education Program Coordinating Committee. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. 2003;289:2560–2572. - PubMed
-
- Lloyd-Jones DM, Evans JC, Larson MG, O'Donnell CJ, Roccella EJ, Levy D. Differential control of systolic and diastolic blood pressure: factors associated with lack of blood pressure control in the community. Hypertension. 2000;36:594–599. - PubMed
-
- Franklin SS, Jacobs MJ, Wong ND, L'Italien GJ, Lapuerta P. Predominance of isolated systolic hypertension among middle-aged and elderly US hypertensives: analysis based on National Health and Nutrition Examination Survey (NHANES) III. Hypertension. 2001;37:869–874. - PubMed
Publication types
MeSH terms
Grants and funding
- 2-K24-HL04334/HL/NHLBI NIH HHS/United States
- R01 HL107385/HL/NHLBI NIH HHS/United States
- R01 HL092577/HL/NHLBI NIH HHS/United States
- N01 HC025195/HC/NHLBI NIH HHS/United States
- T32 HL094300/HL/NHLBI NIH HHS/United States
- R01 HL076784/HL/NHLBI NIH HHS/United States
- R01 HL060040/HL/NHLBI NIH HHS/United States
- HL080124/HL/NHLBI NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- HL076784/HL/NHLBI NIH HHS/United States
- R01 HL080124/HL/NHLBI NIH HHS/United States
- R01 HL070100/HL/NHLBI NIH HHS/United States
- HL071039/HL/NHLBI NIH HHS/United States
- N01-HC-25195/HC/NHLBI NIH HHS/United States
- HL070100/HL/NHLBI NIH HHS/United States
- HL107385/HL/NHLBI NIH HHS/United States
- R01 HL071039/HL/NHLBI NIH HHS/United States
- AG028321/AG/NIA NIH HHS/United States
- HL077447/HL/NHLBI NIH HHS/United States
- K24 HL004334/HL/NHLBI NIH HHS/United States
- R01 HL077447/HL/NHLBI NIH HHS/United States
- 5T32HL094300-05/HL/NHLBI NIH HHS/United States
- R01 AG028321/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
