

A putative placebo analysis of the effects of LCZ696 on clinical outcomes in heart failure
- PMID: 25416329
- PMCID: PMC4328198
- DOI: 10.1093/eurheartj/ehu455
A putative placebo analysis of the effects of LCZ696 on clinical outcomes in heart failure
Abstract
Aims: Although active-controlled trials with renin–angiotensin inhibitors are ethically mandated in heart failure with reduced ejection fraction, clinicians and regulators often want to know how the experimental therapy would perform compared with placebo. The angiotensin receptor-neprilysin inhibitor LCZ696 was compared with enalapril in PARADIGM-HF. We made indirect comparisons of the effects of LCZ696 with putative placebos.
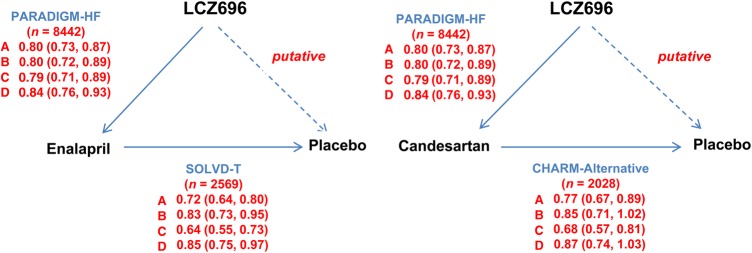
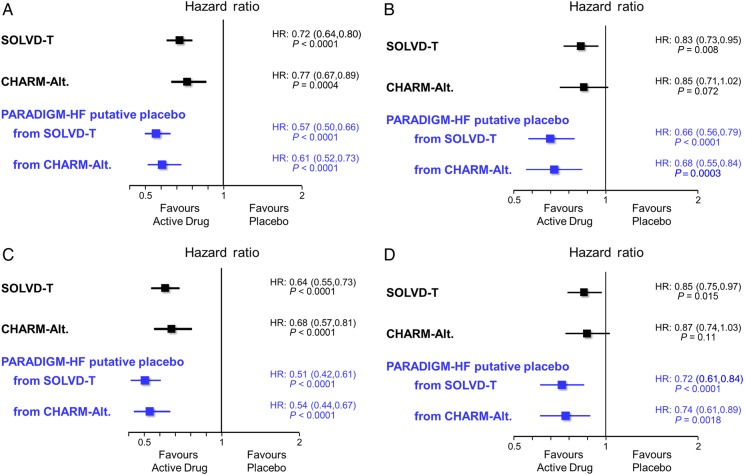
Methods and results: We used the treatment-arm of the Studies Of Left Ventricular Dysfunction (SOLVD-T) as the reference trial for comparison of an ACE inhibitor to placebo and the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity-Alternative trial (CHARM-Alternative) as the reference trial for comparison of an ARB to placebo. The hazard ratio of LCZ696 vs. a putative placebo was estimated through the product of the hazard ratio of LCZ696 vs. enalapril (active-control) and that of the historical active-control (enalapril or candesartan) vs. placebo. For the primary composite outcome of cardiovascular death or heart failure hospitalization in PARADIGM-HF, the relative risk reduction with LCZ696 vs. a putative placebo from SOLVD-T was 43% (95%CI 34–50%; P < 0.0001) with similarly large effects on cardiovascular death (34%, 21–44%; P < 0.0001) and heart failure hospitalization (49%, 39–58%; P < 0.0001). For all-cause mortality, the reduction compared with a putative placebo was 28% (95%CI 15–39%; P < 0.0001). Putative placebo analyses based on CHARM-Alternative gave relative risk reductions of 39% (95%CI 27–48%; P < 0.0001) for the composite outcome of cardiovascular death or heart failure hospitalization, 32% (95%CI 16–45%; P < 0.0001) for cardiovascular death, 46% (33–56%; P < 0.0001) for heart failure hospitalization, and 26% (95%CI 11–39%; P < 0.0001) for all-cause mortality.
Conclusion: These indirect comparisons of LCZ696 with a putative placebo show that the strategy of combined angiotensin receptor blockade and neprilysin inhibition led to striking reductions in cardiovascular and all-cause mortality, as well as heart failure hospitalization. These benefits were obtained even though LCZ696 was added to comprehensive background beta-blocker and mineralocorticoid receptor antagonist therapy.
Trial registration: ClinicalTrials.gov NCT01035255.
Figures
Comment in
-
LCZ696: too good to be true?Eur Heart J. 2015 Feb 14;36(7):410-2. doi: 10.1093/eurheartj/ehu501. Epub 2014 Dec 29. Eur Heart J. 2015. PMID: 25549727 No abstract available.
References
-
- Pitt B, Poole-Wilson PA, Segal R, Martinez FA, Dickstein K, Camm AJ, Konstam MA, Riegger G, Klinger GH, Neaton J, Sharma D, Thiyagarajan B. Effect of losartancompared with captopril on mortality in patients with symptomatic heart failure: randomised trial—the Losartan Heart Failure Survival Study ELITE II. Lancet. 2000;355:1582–1587. - PubMed
-
- Pfeffer MA, McMurray JJ, Velazquez EJ, Rouleau JL, Køber L, Maggioni AP, Solomon SD, Swedberg K, Van de Werf F, White H, Leimberger JD, Henis M, Edwards S, Zelenkofske S, Sellers MA, Califf RM Valsartan in Acute Myocardial Infarction Trial Investigators. Valsartan, captopril, or both in myocardial infarction complicated by heart failure, left ventricular dysfunction, or both. N Engl J Med. 2003;349:1893–1906. Erratum in N Engl J Med 2004;350:203. - PubMed
-
- Dickstein K, Kjekshus J OPTIMAAL Steering Committee of the OPTIMAAL Study Group. Effects of losartan and captopril on mortality and morbidity in high-risk patients after acute myocardial infarction: the OPTIMAAL randomised trial. Optimal Trial in Myocardial Infarction with Angiotensin II Antagonist Losartan. Lancet. 2002;360:752–760. - PubMed
-
- Krum H, Massie B, Abraham WT, Dickstein K, Kober L, McMurray JJ, Desai A, Gimpelewicz C, Kandra A, Reimund B, Rattunde H, Armbrecht J ATMOSPHERE Investigators. Direct renin inhibition in addition to or as an alternative to angiotensin converting enzyme inhibition in patients with chronic systolic heart failure: rationale and design of the Aliskiren Trial to Minimize OutcomeS in Patients with HEart failuRE (ATMOSPHERE) study. Eur J Heart Fail. 2011;13:107–114. - PubMed
-
- McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, Rouleau JL, Shi VC, Solomon SD, Swedberg K, Zile MR PARADIGM-HF Investigators and Committees. Angiotensin–Neprilysin Inhibition versus Enalapril in Heart Failure. N Engl J med. 2014;371:993–1004. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
