

Hypoxia, not pulmonary vascular pressure, induces blood flow through intrapulmonary arteriovenous anastomoses
- PMID: 25416621
- PMCID: PMC4324716
- DOI: 10.1113/jphysiol.2014.282962
Hypoxia, not pulmonary vascular pressure, induces blood flow through intrapulmonary arteriovenous anastomoses
Abstract
Key points: Blood flow through intrapulmonary arteriovenous anastomoses (IPAVA) is increased by acute hypoxia during rest by unknown mechanisms. Oral administration of acetazolamide blunts the pulmonary vascular pressure response to acute hypoxia, thus permitting the observation of IPAVA blood flow with minimal pulmonary pressure change. Hypoxic pulmonary vasoconstriction was attenuated in humans following acetazolamide administration and partially restored with bicarbonate infusion, indicating that the effects of acetazolamide on hypoxic pulmonary vasoconstriction may involve an interaction between arterial pH and PCO2. We observed that IPAVA blood flow during hypoxia was similar before and after acetazolamide administration, even after acid-base status correction, indicating that pulmonary pressure, pH and PCO2 are unlikely regulators of IPAVA blood flow.
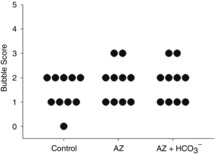
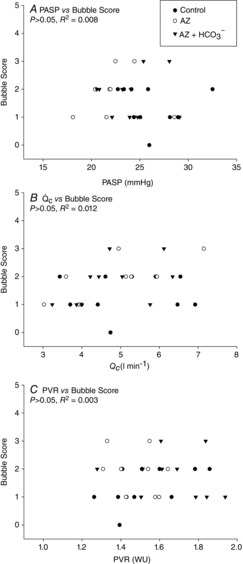
Abstract: Blood flow through intrapulmonary arteriovenous anastomoses (IPAVA) is increased with exposure to acute hypoxia and has been associated with pulmonary artery systolic pressure (PASP). We aimed to determine the direct relationship between blood flow through IPAVA and PASP in 10 participants with no detectable intracardiac shunt by comparing: (1) isocapnic hypoxia (control); (2) isocapnic hypoxia with oral administration of acetazolamide (AZ; 250 mg, three times a day for 48 h) to prevent increases in PASP; and (3) isocapnic hypoxia with AZ and 8.4% NaHCO3 infusion (AZ + HCO3 (-) ) to control for AZ-induced acidosis. Isocapnic hypoxia (20 min) was maintained by end-tidal forcing, blood flow through IPAVA was determined by agitated saline contrast echocardiography and PASP was estimated by Doppler ultrasound. Arterial blood samples were collected at rest before each isocapnic-hypoxia condition to determine pH, [HCO3(-)] and Pa,CO2. AZ decreased pH (-0.08 ± 0.01), [HCO3(-)] (-7.1 ± 0.7 mmol l(-1)) and Pa,CO2 (-4.5 ± 1.4 mmHg; P < 0.01), while intravenous NaHCO3 restored arterial blood gas parameters to control levels. Although PASP increased from baseline in all three hypoxic conditions (P < 0.05), a main effect of condition expressed an 11 ± 2% reduction in PASP from control (P < 0.001) following AZ administration while intravenous NaHCO3 partially restored the PASP response to isocapnic hypoxia. Blood flow through IPAVA increased during exposure to isocapnic hypoxia (P < 0.01) and was unrelated to PASP, cardiac output and pulmonary vascular resistance for all conditions. In conclusion, isocapnic hypoxia induces blood flow through IPAVA independent of changes in PASP and the influence of AZ on the PASP response to isocapnic hypoxia is dependent upon the H(+) concentration or Pa,CO2.
© 2014 The Authors. The Journal of Physiology © 2014 The Physiological Society.
Figures

 , end-tidal partial pressure of oxygen;
, end-tidal partial pressure of oxygen;  , end-tidal partial pressure of carbon dioxide.
, end-tidal partial pressure of carbon dioxide.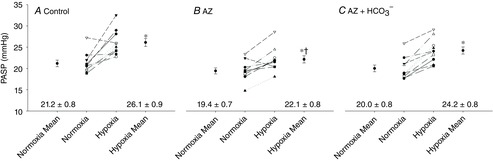
 c, cardiac output.
c, cardiac output.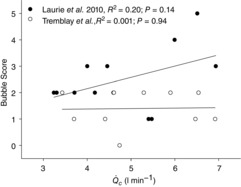
 c obtained during the last minute of exposure to 20 min of isocapnic hypoxia from the current study (n = 10) and poikilocapnic hypoxia from participants in the study by Laurie et al. (2010) (n = 12) breathing 12% O2 for 30 min.
c obtained during the last minute of exposure to 20 min of isocapnic hypoxia from the current study (n = 10) and poikilocapnic hypoxia from participants in the study by Laurie et al. (2010) (n = 12) breathing 12% O2 for 30 min.Similar articles
-
Intrapulmonary arteriovenous anastomoses in humans--response to exercise and the environment.J Physiol. 2015 Feb 1;593(3):507-20. doi: 10.1113/jphysiol.2014.275495. Epub 2015 Jan 7. J Physiol. 2015. PMID: 25565568 Free PMC article. Review.
-
Sildenafil, nifedipine and acetazolamide do not allow for blood flow through intrapulmonary arteriovenous anastomoses during exercise while breathing 100% oxygen.Exp Physiol. 2014 Dec 1;99(12):1636-47. doi: 10.1113/expphysiol.2014.081562. Epub 2014 Sep 25. Exp Physiol. 2014. PMID: 25261497
-
Catecholamine-induced opening of intrapulmonary arteriovenous anastomoses in healthy humans at rest.J Appl Physiol (1985). 2012 Oct 15;113(8):1213-22. doi: 10.1152/japplphysiol.00565.2012. Epub 2012 Aug 2. J Appl Physiol (1985). 2012. PMID: 22858627
-
Resting pulmonary haemodynamics and shunting: a comparison of sea-level inhabitants to high altitude Sherpas.J Physiol. 2014 Mar 15;592(6):1397-409. doi: 10.1113/jphysiol.2013.266593. Epub 2014 Jan 6. J Physiol. 2014. PMID: 24396057 Free PMC article.
-
Carbonic anhydrase inhibitors and hypoxic pulmonary vasoconstriction.Respir Physiol Neurobiol. 2006 Apr 28;151(2-3):209-16. doi: 10.1016/j.resp.2005.10.011. Epub 2005 Dec 20. Respir Physiol Neurobiol. 2006. PMID: 16376158 Review.
Cited by
-
Intrapulmonary arteriovenous anastomoses in humans--response to exercise and the environment.J Physiol. 2015 Feb 1;593(3):507-20. doi: 10.1113/jphysiol.2014.275495. Epub 2015 Jan 7. J Physiol. 2015. PMID: 25565568 Free PMC article. Review.
-
Decreased arterial PO2, not O2 content, increases blood flow through intrapulmonary arteriovenous anastomoses at rest.J Physiol. 2016 Sep 1;594(17):4981-96. doi: 10.1113/JP272211. Epub 2016 Jun 9. J Physiol. 2016. PMID: 27062157 Free PMC article. Clinical Trial.
-
Ventilatory responses to acute hypoxia and hypercapnia in humans with a patent foramen ovale.J Appl Physiol (1985). 2019 Mar 1;126(3):730-738. doi: 10.1152/japplphysiol.00741.2018. Epub 2018 Dec 6. J Appl Physiol (1985). 2019. PMID: 30521423 Free PMC article. Clinical Trial.
-
Evaluation of intrapulmonary arteriovenous anastomoses before and after oxygen supplementation, using transthoracic agitated saline contrast echocardiography in rescued Korean raccoon dogs.Front Vet Sci. 2024 Aug 8;11:1362363. doi: 10.3389/fvets.2024.1362363. eCollection 2024. Front Vet Sci. 2024. PMID: 39176393 Free PMC article.
-
UBC-Nepal Expedition: acute alterations in sympathetic nervous activity do not influence brachial artery endothelial function at sea level and high altitude.J Appl Physiol (1985). 2017 Nov 1;123(5):1386-1396. doi: 10.1152/japplphysiol.00583.2017. Epub 2017 Aug 31. J Appl Physiol (1985). 2017. PMID: 28860174 Free PMC article. Clinical Trial.
References
-
- Abbas AE, Fortuin FD, Schiller NB, Appleton CP, Moreno CA. Lester SJ. A simple method for noninvasive estimation of pulmonary vascular resistance. J Am Coll Cardiol. 2003;41:1021–1027. - PubMed
-
- Albert TJ. Swenson ER. Peripheral chemoreceptor responsiveness and hypoxic pulmonary vasoconstriction in humans. High Alt Med Biol. 2014;15:15–20. - PubMed
-
-
Bain AR, Smith KJ, Lewis NC, Foster GE, Wildfong KW, Willie CK, Hartley GL, Cheung SS. Ainslie PN. Regional changes in brain blood flow during severe passive hyperthermia: effects of
 and extracranial blood flow. J Appl Physiol. 2013;115:653–659.
-
PubMed
and extracranial blood flow. J Appl Physiol. 2013;115:653–659.
-
PubMed
-
Bain AR, Smith KJ, Lewis NC, Foster GE, Wildfong KW, Willie CK, Hartley GL, Cheung SS. Ainslie PN. Regional changes in brain blood flow during severe passive hyperthermia: effects of
-
- Balanos GM, Talbot NP, Dorrington KL. Robbins PA. Human pulmonary vascular response to 4 h of hypercapnia and hypocapnia measured using Doppler echocardiography. J Appl Physiol. 2003;94:1543–1551. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources