

Heterogeneous associations between smoking and a wide range of initial presentations of cardiovascular disease in 1937360 people in England: lifetime risks and implications for risk prediction
- PMID: 25416721
- PMCID: PMC4339760
- DOI: 10.1093/ije/dyu218
Heterogeneous associations between smoking and a wide range of initial presentations of cardiovascular disease in 1937360 people in England: lifetime risks and implications for risk prediction
Abstract
Background: It is not known how smoking affects the initial presentation of a wide range of chronic and acute cardiovascular diseases (CVDs), nor the extent to which associations are heterogeneous. We estimated the lifetime cumulative incidence of 12 CVD presentations, and examined associations with smoking and smoking cessation.
Methods: Cohort study of 1.93 million people aged ≥30years, with no history of CVD, in 1997-2010. Individuals were drawn from linked electronic health records in England, covering primary care, hospitalizations, myocardial infarction (MI) registry and cause-specific mortality (the CALIBER programme).
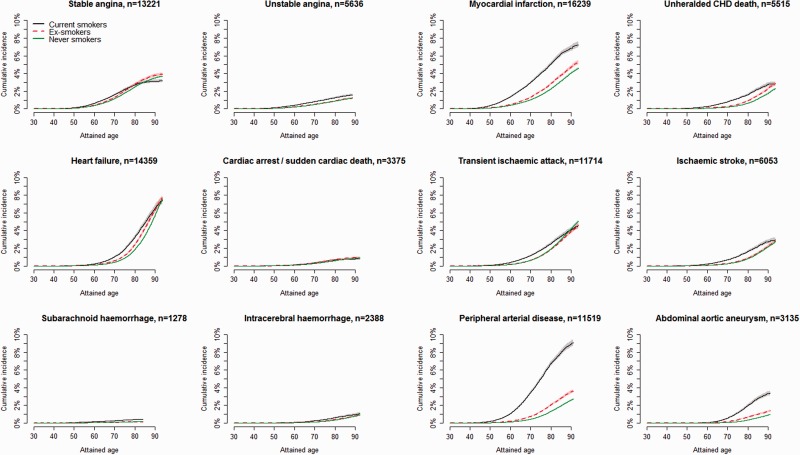
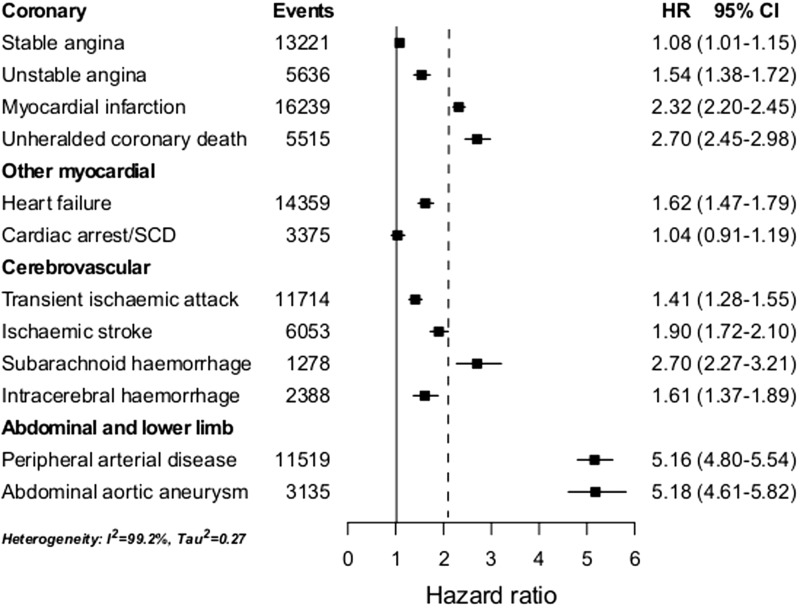
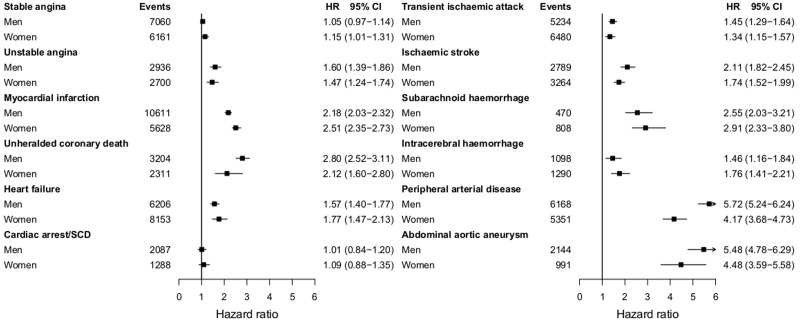
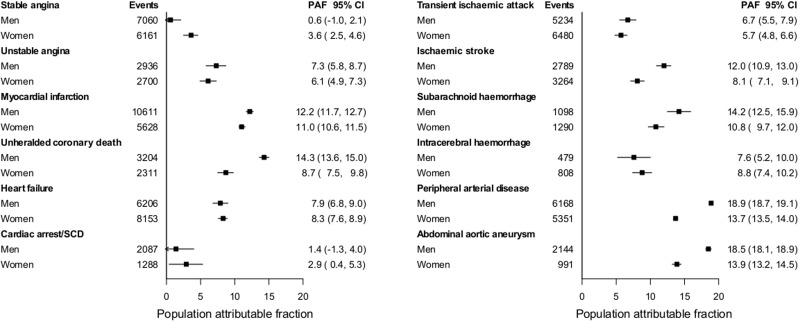
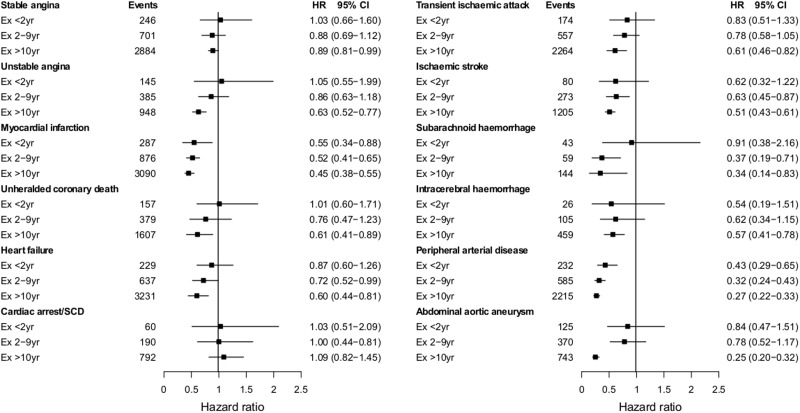
Results: During 11.6 million person-years of follow-up, 114859 people had an initial non-fatal or fatal CVD presentation. By age 90 years, current vs never smokers' lifetime risks varied from 0.4% vs 0.2% for subarachnoid haemorrhage (SAH), to 8.9% vs 2.6% for peripheral arterial disease (PAD). Current smoking showed no association with cardiac arrest or sudden cardiac death [hazard ratio (HR)=1.04, 95% confidence interval (CI) 0.91-1.19).The strength of association differed markedly according to disease type: stable angina (HR=1.08, 95% CI 1.01-1.15),transient ischaemic attack (HR=1.41, 95% CI 1.28-1.55), unstable angina (HR=1.54, 95% CI 1.38-1.72), intracerebral haemorrhage (HR=1.61, 95% CI 1.37-1.89), heart failure (HR=1.62, 95% CI 1.47-1.79), ischaemic stroke (HR=1.90, 95% CI 1.72-2.10), MI (HR=2.32, 95% CI 2.20-2.45), SAH (HR= 2.70, 95% CI 2.27-3.21), PAD (HR=5.16, 95% CI 4.80-5.54) and abdominal aortic aneurysm (AAA) (HR=5.18, 95% CI 4.61-5.82). Population-attributable fractions were lower for women than men for unheralded coronary death, ischaemic stroke, PAD and AAA. Ten years after quitting smoking, the risks of PAD, AAA (in men) and unheralded coronary death remained increased (HR=1.36, 1.47 and 2.74, respectively).
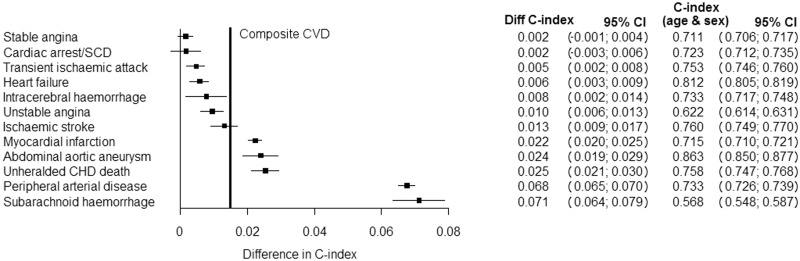
Conclusions: The heterogeneous associations of smoking with different CVD presentations suggests different underlying mechanisms and have important implications for research, clinical screening and risk prediction.
Keywords: Association study; cardiovascular outcomes; epidemiology; initial presentation; lifetime risks; primary prevention; risk prediction; risk stratification; smoking.
© The Author 2014; all rights reserved. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures
References
-
- Critchley J, Capewell S. Smoking cessation for the secondary prevention of coronary heart disease. Cochrane DatabaseSyst Rev 2004;1:CD003041. - PubMed
-
- Mackay DF, Irfan MO, Haw S, Pell JP. Meta-analysis of the effect of comprehensive smoke-free legislation on acute coronary events. Heart 2010;96:1525–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
