

When do changes in cancer survival mean progress? The insight from population incidence and mortality
- PMID: 25417232
- PMCID: PMC4841163
- DOI: 10.1093/jncimonographs/lgu014
When do changes in cancer survival mean progress? The insight from population incidence and mortality
Abstract
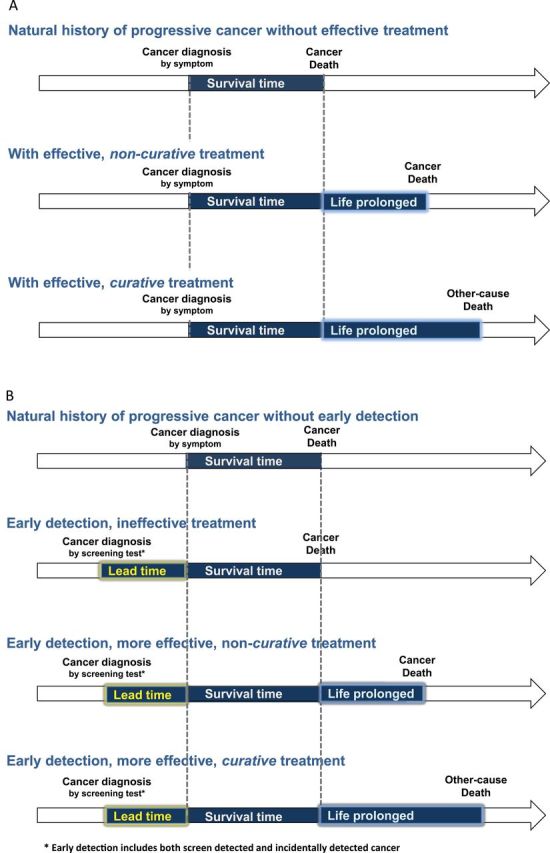
Background: It is often assumed that increases in cancer survival reflect true progress against cancer. This is true when these increases are accompanied by decreased burden of disease: Fewer people being diagnosed or dying from cancer (ie, decreased incidence and mortality). But increased survival can also occur even when incidence is increasing and mortality is unchanged.
Objective: To use trends in cancer burden-incidence and mortality-to illustrate when changes in survival reflect true progress.
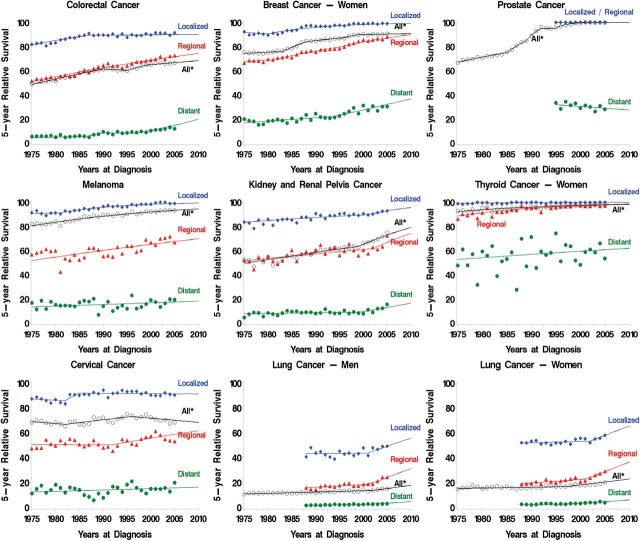
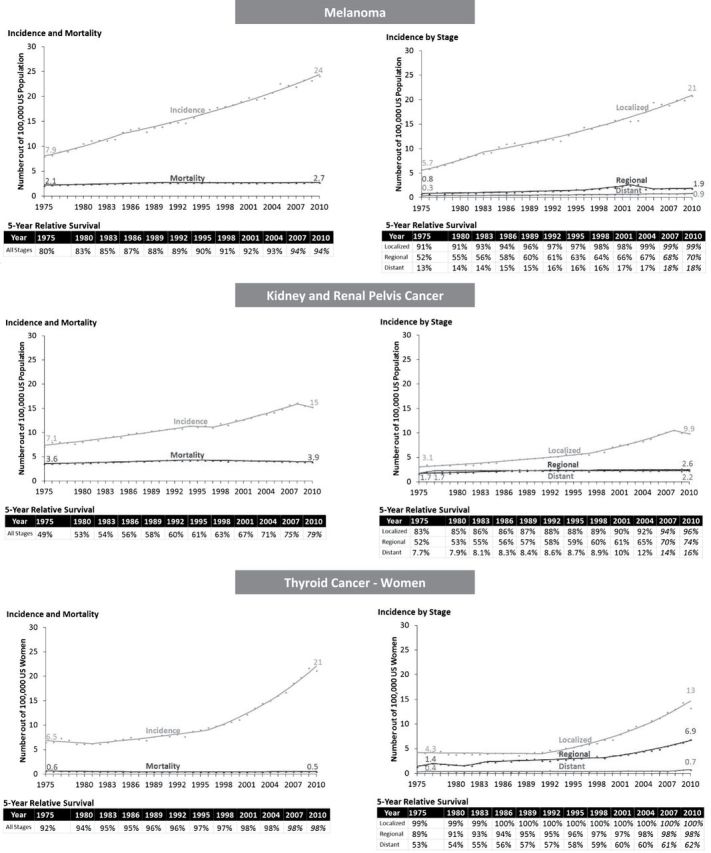
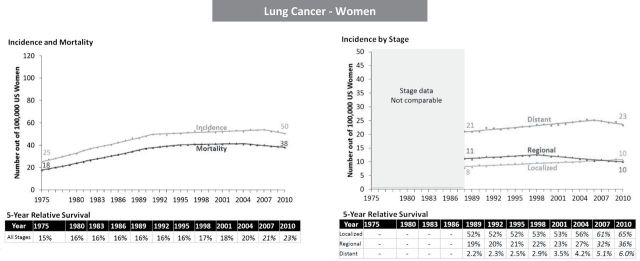
Methods: Using data from 1975 to 2010 collected by the Surveillance, Epidemiology, and End Results Program (incidence, survival) and the National Center for Health Statistics (mortality), we analyzed US trends in five-year relative survival, age-adjusted incidence, and mortality for selected cancers to identify patterns that do and do not reflect progress.
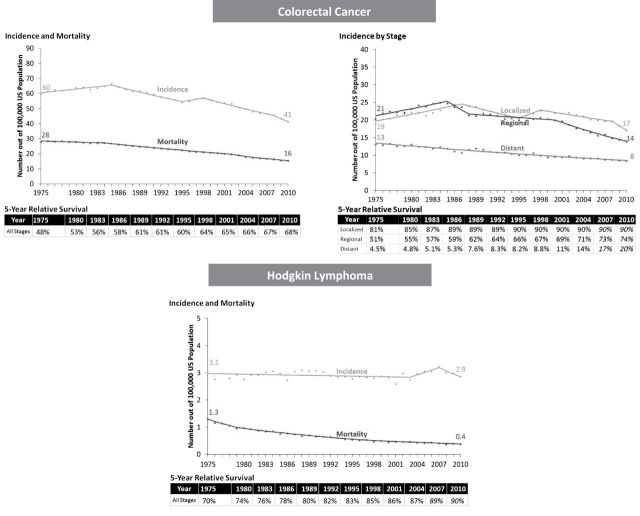
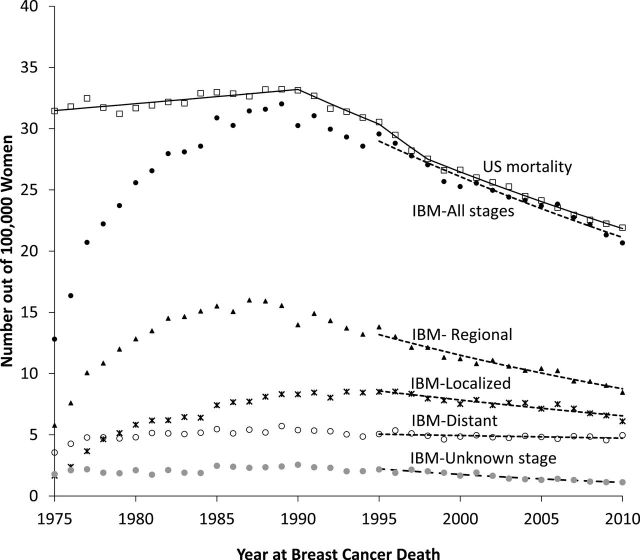
Results: Among the nine common cancers examined, survival increased in seven, and changed little or not at all for two. In some cases, increased survival was accompanied by decreased burden of disease, reflecting true progress. For example, from 1975 to 2010, five-year survival for colon cancer patients improved (from 48% to 68%) while cancer burden fell: Fewer cases (incidence decreased from 60 to 41 per 100,000) and fewer deaths (mortality decreased from 28 to 16 per 100,000), a pattern explained by both increased early detection (with removal of cancer precursors) and more effective treatment. In other cases, however, increased survival did not reflect true progress. In melanoma, kidney, and thyroid cancer, five-year survival increased but incidence increased with no change in mortality. This pattern suggests overdiagnosis from increased early detection, an increase in cancer burden.
Conclusions: Changes in survival must be interpreted in the context of incidence and mortality. Increased survival only represents progress when accompanied by a reduction in incidence, mortality, or ideally both.
Published by Oxford University Press 2014.
Figures
References
-
- Woloshin S, Schwartz LM. How a charity oversells mammography. BMJ. 2012;345:e5132. - PubMed
-
- Dickman PW, Adami HO. Interpreting trends in cancer patient survival. J Intern Med. 2006;260(2):103–117. - PubMed
-
- Chu KC, Miller BA, Feuer EJ, Hankey BF. A method for partitioning cancer mortality trends by factors associated with diagnosis: an application to female breast cancer. J Clin Epidemiol. 1994;47(12):1451–1461. - PubMed
-
- Joinpoint: Joinpoint Regression Program [computer program]. Version 4.0.4. http://surveillance.cancer.gov/joinpoint/ Bethesda, MD: Surveillance Research Program, National Cancer Institute; 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
