

Replication and shedding of MERS-CoV in upper respiratory tract of inoculated dromedary camels
- PMID: 25418529
- PMCID: PMC4257817
- DOI: 10.3201/eid2012.141280
Replication and shedding of MERS-CoV in upper respiratory tract of inoculated dromedary camels
Abstract
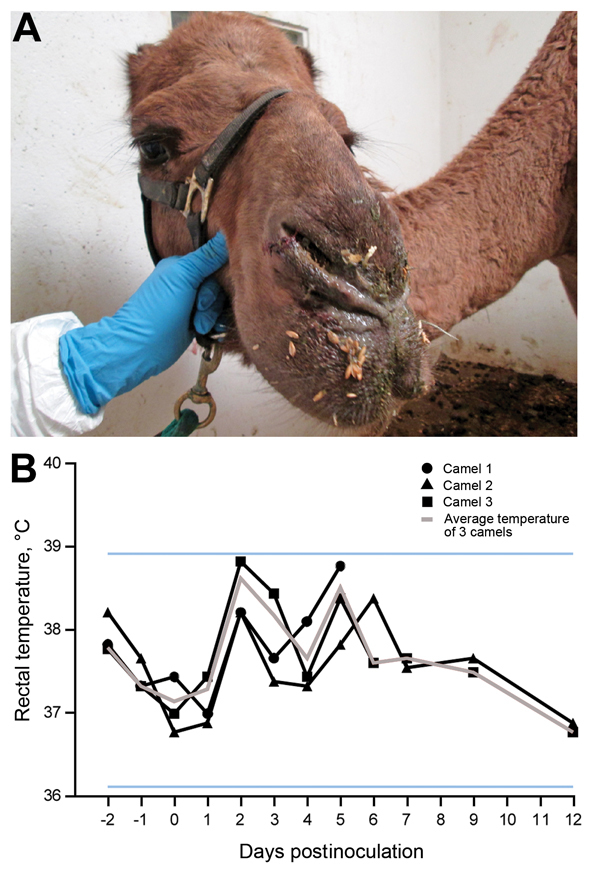
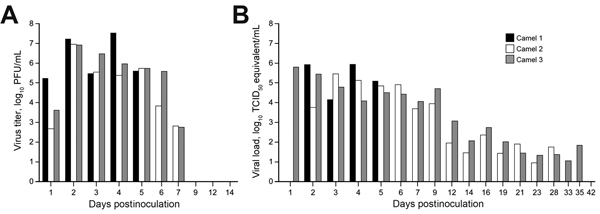
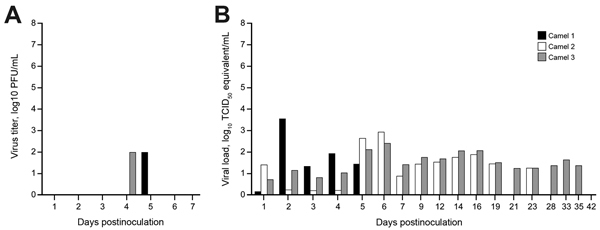
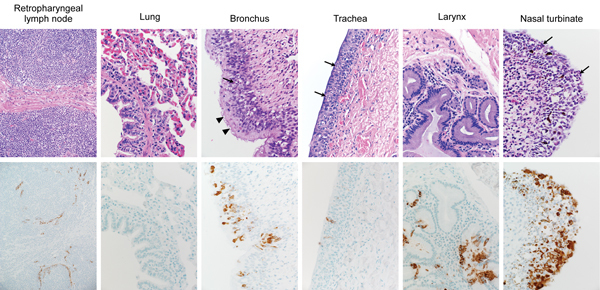
In 2012, a novel coronavirus associated with severe respiratory disease in humans emerged in the Middle East. Epidemiologic investigations identified dromedary camels as the likely source of zoonotic transmission of Middle East respiratory syndrome coronavirus (MERS-CoV). Here we provide experimental support for camels as a reservoir for MERS-CoV. We inoculated 3 adult camels with a human isolate of MERS-CoV and a transient, primarily upper respiratory tract infection developed in each of the 3 animals. Clinical signs of the MERS-CoV infection were benign, but each of the camels shed large quantities of virus from the upper respiratory tract. We detected infectious virus in nasal secretions through 7 days postinoculation, and viral RNA up to 35 days postinoculation. The pattern of shedding and propensity for the upper respiratory tract infection in dromedary camels may help explain the lack of systemic illness among naturally infected camels and the means of efficient camel-to-camel and camel-to-human transmission.
Figures
References
-
- World Health Organization. Global Alert and Response. Middle East respiratory syndrome coronavirus (MERS-CoV) – update; 2014. June [cited 30 Jun 2014]. <ext-link xmlns:xlink="http://www.w3.org/1999/xlink" ext-link-type="uri" xlink:href="http://www.who.int/csr/don/2014_06_16_mers/en/">http://www.who.int/csr/don/2014_06_16_mers/en<underline>/</underline></ext-link>
-
- Puzelli S, Azzi A, Santini MG, Di Martino A, Facchini M, Castrucci MR, et al. Investigation of an imported case of Middle East respiratory syndrome coronavirus (MERS-CoV) infection in Florence, Italy, May to June 2013. Euro Surveill. 2013;18:20564 . - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
