

Implementing Behavioral Activation and Life-Steps for Depression and HIV Medication Adherence in a Community Health Center
- PMID: 25419102
- PMCID: PMC4238929
- DOI: 10.1016/j.cbpra.2013.10.002
Implementing Behavioral Activation and Life-Steps for Depression and HIV Medication Adherence in a Community Health Center
Abstract
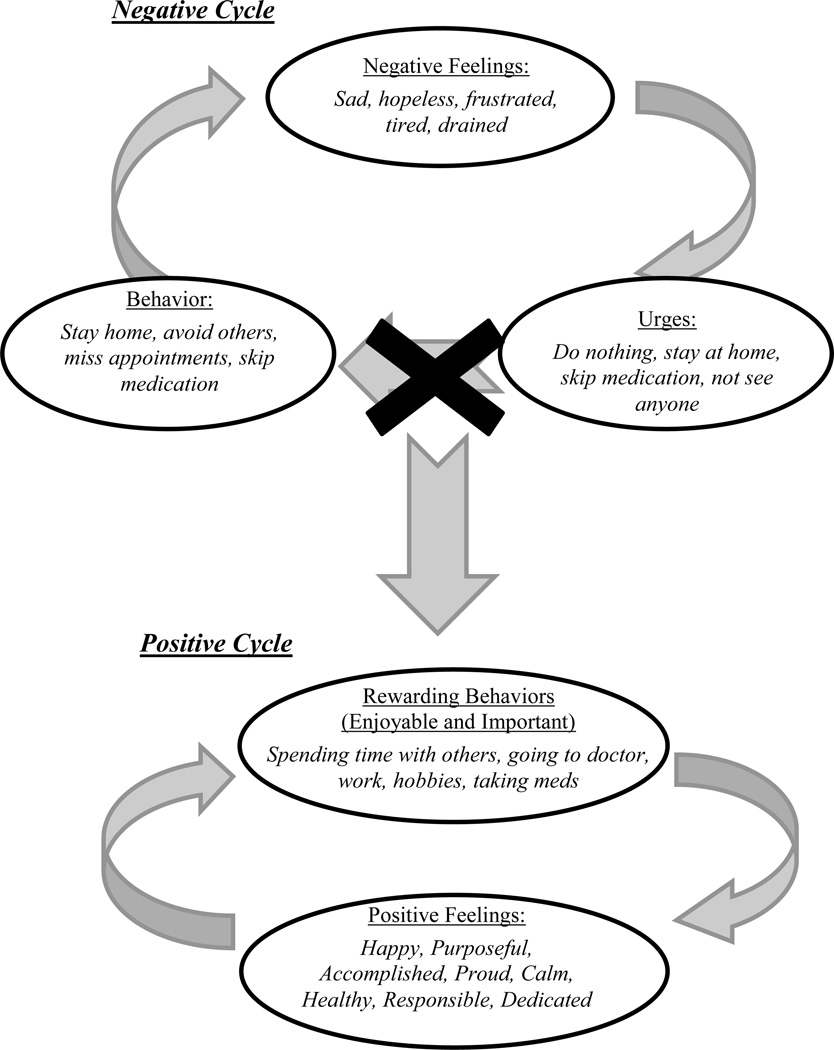
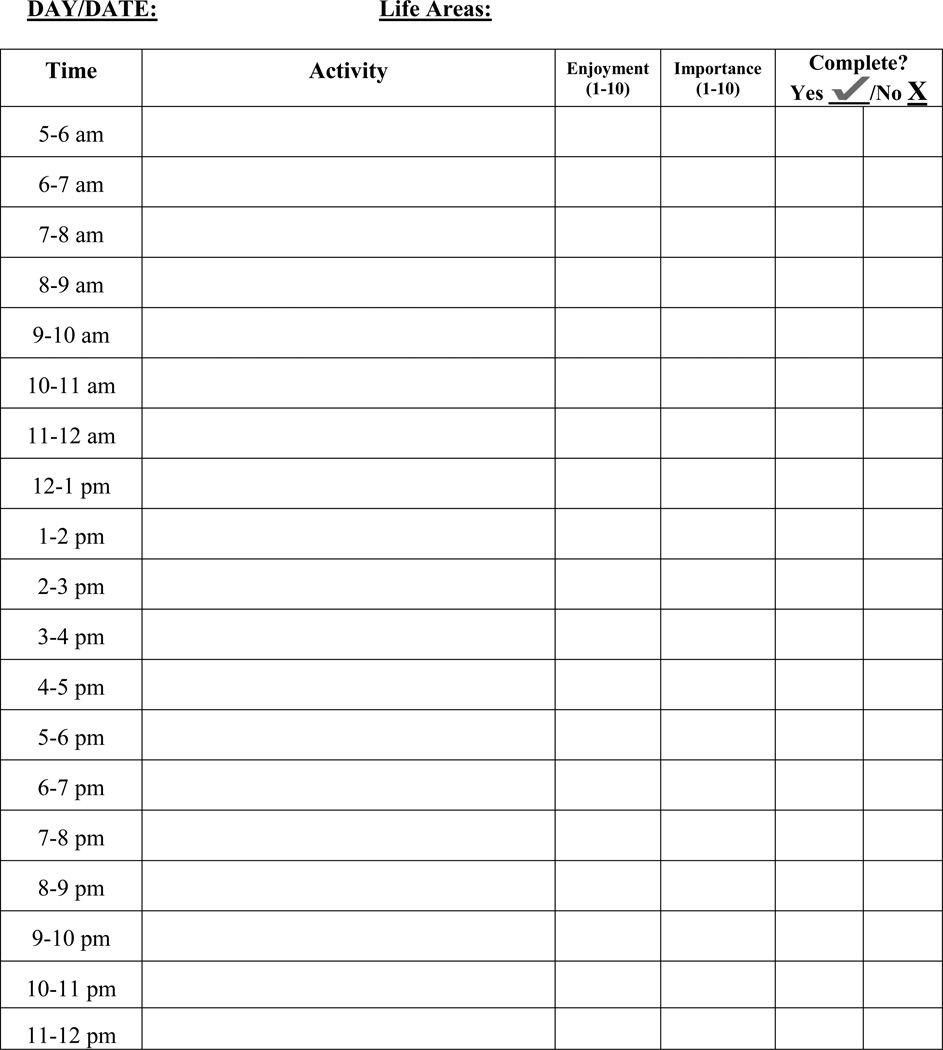
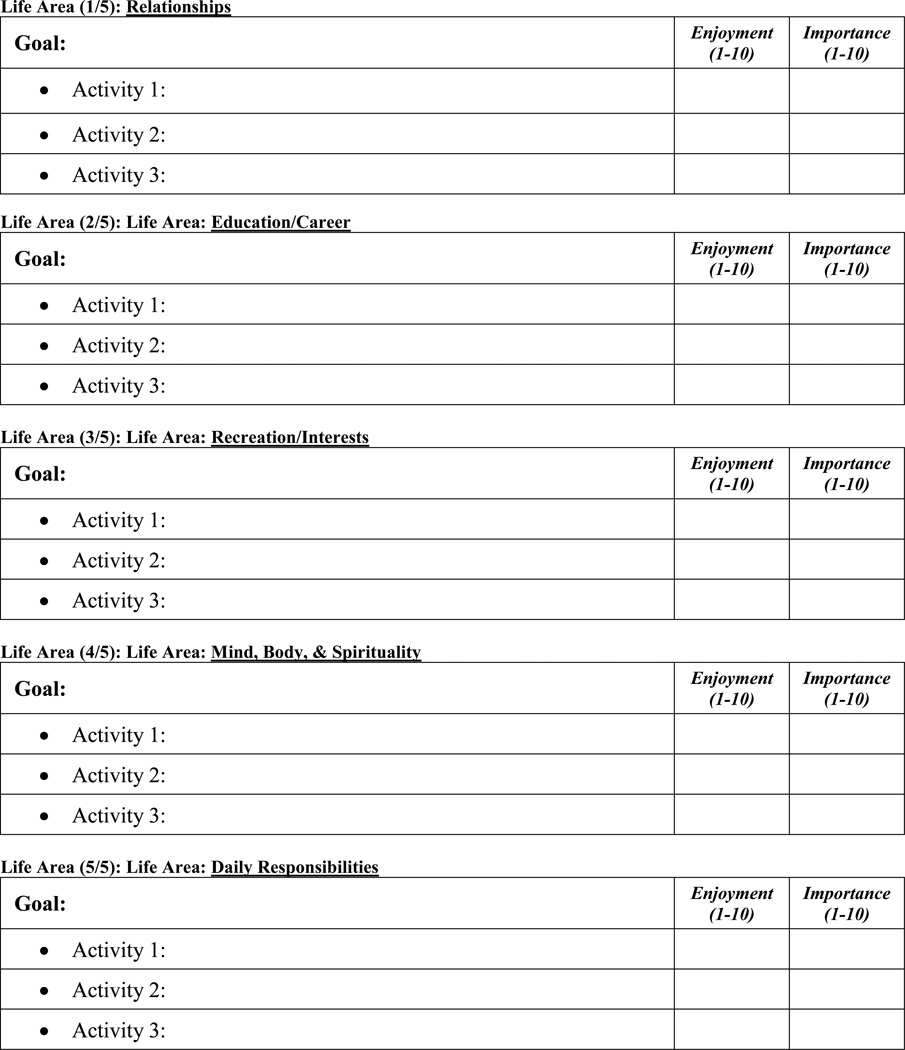
Antiretroviral therapy to treat HIV/AIDS has substantially improved clinical outcomes among patients living with HIV/AIDS, but only in the presence of very consistent adherence. One of the most prevalent and impactful individual-level predictors of poor adherence is depressive symptoms, even at subthreshold levels. Evidence-based cognitive behavioral interventions exist to address improvements in depressive symptoms and adherence in this population, yet these techniques have largely been designed and tested as individual treatments for delivery in mental health settings. This presents a significant challenge when transporting these techniques to medical settings where other formats for delivery may be more appropriate (i.e., groups, less frequent visits) and few hands-on resources exist to guide this process. As such, primary aims of this study were to adapt and implement evidence-based cognitive behavioral techniques for depression (behavioral activation; BA) and HIV medication adherence (Life-Steps) that have potential for dissemination in an outpatient community health center. The intervention incorporated feedback from health center staff and utilized a modular, group format that did not rely on sequential session attendance. Feasibility was examined over 8 weeks (n = 13). Preliminary effects on depression, health-related quality of life, and medication adherence were examined and exit interviews were conducted with a subset of participants (n = 4) to inform future modifications. Treatment descriptions and recommendations for effective clinical implementation based on patient and clinician feedback are provided along with case material of two individual patients and an example group session. Current efforts are an important next step for disseminating evidence-based techniques for depression and HIV medication adherence to community health center or AIDS service organization settings.
Keywords: CBT; HIV medication adherence; behavioral activation; community health center; depression.
Figures
Similar articles
-
Description and Demonstration of Cognitive Behavioral Therapy to Enhance Antiretroviral Therapy Adherence and Treat Depression in HIV-Infected Adults.Cogn Behav Pract. 2015 Nov 1;22(4):430-438. doi: 10.1016/j.cbpra.2014.02.001. Cogn Behav Pract. 2015. PMID: 26688659 Free PMC article.
-
Adherence intervention for HIV-infected persons who use drugs: adaptation, open trial, and pilot randomized hybrid type 1 trial protocol.Addict Sci Clin Pract. 2018 Apr 2;13(1):12. doi: 10.1186/s13722-018-0113-5. Addict Sci Clin Pract. 2018. PMID: 29606129 Free PMC article. Clinical Trial.
-
An Initial Open Trial of a Brief Behavioral Activation Treatment for Depression and Medication Adherence in HIV-Infected Patients.Behav Modif. 2018 Mar;42(2):196-209. doi: 10.1177/0145445517723901. Epub 2017 Aug 11. Behav Modif. 2018. PMID: 28799413
-
Nonsomatic treatment of depression.Child Adolesc Psychiatr Clin N Am. 2002 Jul;11(3):579-93. doi: 10.1016/s1056-4993(02)00009-3. Child Adolesc Psychiatr Clin N Am. 2002. PMID: 12222084 Review.
-
Development and Implementation of Health and Wellness CBT for Individuals with Depression and HIV.Cogn Behav Pract. 2014 May;21(2):237-246. doi: 10.1016/j.cbpra.2013.07.003. Cogn Behav Pract. 2014. PMID: 24795524 Free PMC article.
Cited by
-
Feasibility, Acceptability, and Preliminary Effectiveness of a 4-week Mindfulness-Based Cognitive Therapy Protocol for Hospital Employees.Mindfulness (N Y). 2017 Dec;8(6):1522-1531. doi: 10.1007/s12671-017-0718-x. Epub 2017 Apr 1. Mindfulness (N Y). 2017. PMID: 29335671 Free PMC article.
-
Barriers and facilitators of interventions for improving antiretroviral therapy adherence: a systematic review of global qualitative evidence.J Int AIDS Soc. 2016 Oct 17;19(1):21166. doi: 10.7448/IAS.19.1.21166. eCollection 2016. J Int AIDS Soc. 2016. PMID: 27756450 Free PMC article.
-
"HEAL together": a randomized, hybrid type 1 effectiveness-implementation trial protocol of a peer-delivered behavioral activation intervention to improve methadone treatment retention.Front Public Health. 2025 Jul 18;13:1637846. doi: 10.3389/fpubh.2025.1637846. eCollection 2025. Front Public Health. 2025. PMID: 40756389 Free PMC article.
-
Patient and provider perceptions of a peer-delivered intervention ('Khanya') to improve anti-retroviral adherence and substance use in South Africa: a mixed methods analysis.Glob Ment Health (Camb). 2022 Aug 26;9:439-447. doi: 10.1017/gmh.2022.47. eCollection 2022. Glob Ment Health (Camb). 2022. PMID: 36618732 Free PMC article.
-
A need for implementation science to optimise the use of evidence-based interventions in HIV care: A systematic literature review.PLoS One. 2019 Aug 19;14(8):e0220060. doi: 10.1371/journal.pone.0220060. eCollection 2019. PLoS One. 2019. PMID: 31425524 Free PMC article.
References
-
- Aharonovich E, Hasin DS, Brooks AC, Liu X, Bisaga A, Nunes EV. Cognitive deficits predict low treatment retention in cocaine dependent patients. Drug and Alcohol Dependence. 2006;81(3):313–322. - PubMed
-
- Bangsberg DR, Perry S, Charlebois ED, Clark RA, Roberston M, Zolopa AR, Moss A. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. AIDS. 2001;15(9):1181–1183. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials