

Outcomes after out-of-hospital cardiac arrest treated by basic vs advanced life support
- PMID: 25419698
- PMCID: PMC4314335
- DOI: 10.1001/jamainternmed.2014.5420
Outcomes after out-of-hospital cardiac arrest treated by basic vs advanced life support
Abstract
Importance: Most out-of-hospital cardiac arrests receiving emergency medical services in the United States are treated by ambulance service providers trained in advanced life support (ALS), but supporting evidence for the use of ALS over basic life support (BLS) is limited.
Objective: To compare the effects of BLS and ALS on outcomes after out-of-hospital cardiac arrest.
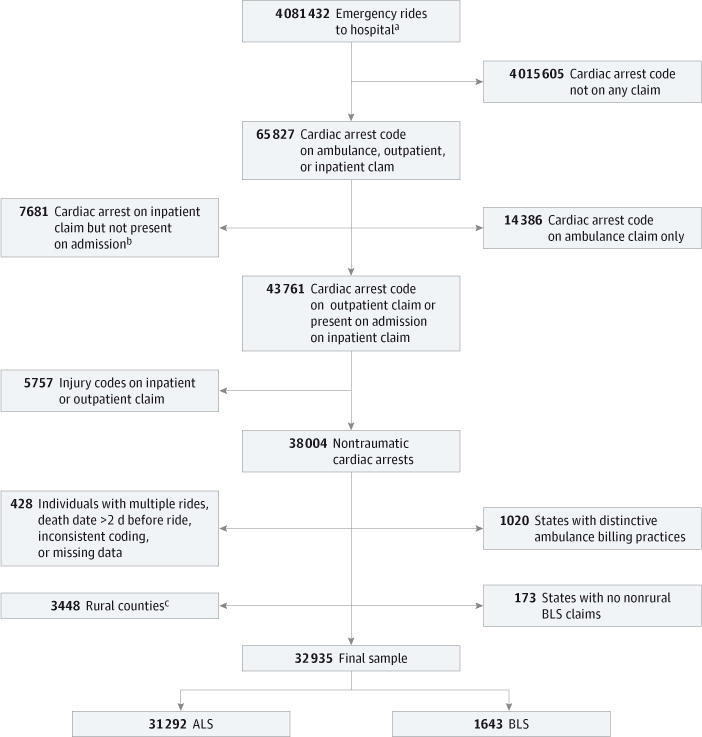
Design, setting, and participants: Observational cohort study of a nationally representative sample of traditional Medicare beneficiaries from nonrural counties who experienced out-of-hospital cardiac arrest between January 1, 2009, and October 2, 2011, and for whom ALS or BLS ambulance services were billed to Medicare (31,292 ALS cases and 1643 BLS cases). Propensity score methods were used to compare the effects of ALS and BLS on patient survival, neurological performance, and medical spending after cardiac arrest.
Main outcomes and measures: Survival to hospital discharge, to 30 days, and to 90 days; neurological performance; and incremental medical spending per additional survivor to 1 year.
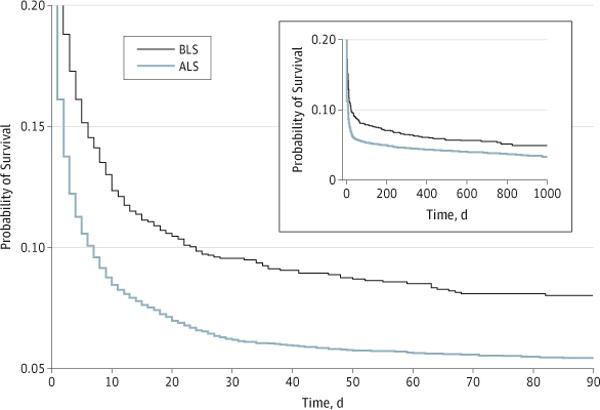
Results: Survival to hospital discharge was greater among patients receiving BLS (13.1% vs 9.2% for ALS; 4.0 [95% CI, 2.3-5.7] percentage point difference), as was survival to 90 days (8.0% vs 5.4% for ALS; 2.6 [95% CI, 1.2-4.0] percentage point difference). Basic life support was associated with better neurological functioning among hospitalized patients (21.8% vs 44.8% with poor neurological functioning for ALS; 23.0 [95% CI, 18.6-27.4] percentage point difference). Incremental medical spending per additional survivor to 1 year for BLS relative to ALS was $154,333.
Conclusions and relevance: Patients with out-of-hospital cardiac arrest who received BLS had higher survival at hospital discharge and at 90 days compared with those who received ALS and were less likely to experience poor neurological functioning.
Conflict of interest statement
Figures
Comment in
-
Evidence in support of a back-to-basics approach in out-of-hospital cardiopulmonary resuscitation vs "advanced" treatment.JAMA Intern Med. 2015 Feb;175(2):205-6. doi: 10.1001/jamainternmed.2014.6590. JAMA Intern Med. 2015. PMID: 25420113 No abstract available.
-
Outcomes After Out-of-Hospital Cardiac Arrest Treated by Basic vs Advanced Life Support.JAMA Intern Med. 2015 Aug;175(8):1421. doi: 10.1001/jamainternmed.2015.2097. JAMA Intern Med. 2015. PMID: 26236974 No abstract available.
-
Outcomes After Out-of-Hospital Cardiac Arrest Treated by Basic vs Advanced Life Support.JAMA Intern Med. 2015 Aug;175(8):1421-2. doi: 10.1001/jamainternmed.2015.2103. JAMA Intern Med. 2015. PMID: 26236975 No abstract available.
-
Outcomes After Out-of-Hospital Cardiac Arrest Treated by Basic vs Advanced Life Support.JAMA Intern Med. 2015 Aug;175(8):1422-3. doi: 10.1001/jamainternmed.2015.2109. JAMA Intern Med. 2015. PMID: 26236976 No abstract available.
-
Basic vs Advanced Life Support for Out-of-Hospital Cardiac Arrest--Reply.JAMA Intern Med. 2015 Aug;175(8):1423. doi: 10.1001/jamainternmed.2015.2112. JAMA Intern Med. 2015. PMID: 26236978 No abstract available.
References
-
- Roger VL, Go AS, Lloyd-Jones DM, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics: 2012 update: a report from the American Heart Association [published correction appears in Circulation. 2012;125(22):e1002] Circulation. 2012;125(1):e2–e220. doi: 10.1161/CIR.0b013e31823ac046. - DOI - PMC - PubMed
-
- Hallstrom AP, Ornato JP, Weisfeldt M, et al. Public Access Defibrillation Trial Investigators Public-access defibrillation and survival after out-of-hospital cardiac arrest. N Engl J Med. 2004;351(7):637–646. - PubMed
-
- Stiell IG, Wells GA, Field BJ, III, et al. Improved out-of-hospital cardiac arrest survival through the inexpensive optimization of an existing defibrillation program: OPALS study phase II: Ontario Prehospital Advanced Life Support. JAMA. 1999;281(13):1175–1181. - PubMed
-
- Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346(8):557–563. - PubMed
-
- Hypothermia After Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346(8):549–556. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
