

Pulmonary arteriovenous malformations
- PMID: 25420112
- PMCID: PMC4315816
- DOI: 10.1164/rccm.201407-1254CI
Pulmonary arteriovenous malformations
Abstract
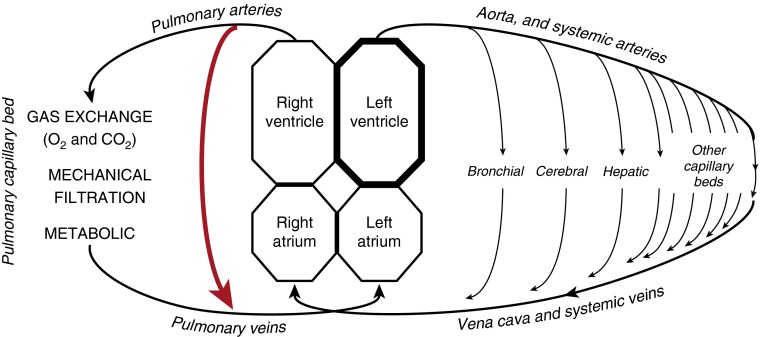
Within the past decade, pulmonary arteriovenous malformations (PAVMs) have evolved from rare curiosities to not uncommon clinical states, with the latest estimates suggesting a prevalence of ~1 in 2,600. PAVMs provide anatomic right-to-left shunts, allowing systemic venous blood to bypass gas exchange and pulmonary capillary bed processing. Hypoxemia and enhanced ventilatory demands result, although both are usually asymptomatic. Paradoxical emboli lead to strokes and cerebral abscesses, and these commonly occur in individuals with previously undiagnosed PAVMs. PAVM hemorrhage is rare but is the main cause of maternal death in pregnancy. PAVM occlusion by embolization is the standard of care to reduce these risks. However, recent data demonstrate that currently recommended management protocols can result in levels of radiation exposure that would be classified as harmful. Recent publications also provide a better appreciation of the hematologic and cardiovascular demands required to maintain arterial oxygen content and oxygen consumption in hypoxemic patients, identify patient subgroups at higher risk of complications, and emphasize the proportion of radiologically visible PAVMs too small to treat by embolization. This review, therefore, outlines medical states that exacerbate the consequences of PAVMs. Chief among these is iron deficiency, which is commonly present due to concurrent hereditary hemorrhagic telangiectasia: iron deficiency impairs hypoxemia compensations by restricting erythropoiesis and increases the risk of ischemic strokes. Management of periodontal disease, dental interventions, pulmonary hypertension, and pregnancy also requires specific consideration in the setting of PAVMs. The review concludes by discussing to what extent previously recommended protocols may benefit from modification or revision.
Keywords: HHT; embolization; hypoxemia/hypoxia; iron deficiency; radiation.
Figures
References
-
- Nakayama M, Nawa T, Chonan T, Endo K, Morikawa S, Bando M, Wada Y, Shioya T, Sugiyama Y, Fukai S. Prevalence of pulmonary arteriovenous malformations as estimated by low-dose thoracic CT screening. Intern Med. 2012;51:1677–1681. - PubMed
-
- Gossage JR, Kanj G. Pulmonary arteriovenous malformations: a state of the art review. Am J Respir Crit Care Med. 1998;158:643–661. - PubMed
-
- Cottin V, Chinet T, Lavolé A, Corre R, Marchand E, Reynaud-Gaubert M, Plauchu H, Cordier JF Groupe d’Etudes et de Recherche sur les Maladies “Orphelines” Pulmonaires (GERM”O”P) Pulmonary arteriovenous malformations in hereditary hemorrhagic telangiectasia: a series of 126 patients. Medicine (Baltimore) 2007;86:1–17. - PubMed
-
- Faughnan ME, Palda VA, Garcia-Tsao G, Geisthoff UW, McDonald J, Proctor DD, Spears J, Brown DH, Buscarini E, Chesnutt MS, et al. HHT Foundation International - Guidelines Working Group. International guidelines for the diagnosis and management of hereditary haemorrhagic telangiectasia. J Med Genet. 2011;48:73–87. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
