

In-home fortification with 2.5 mg iron as NaFeEDTA does not reduce anaemia but increases weight gain: a randomised controlled trial in Kenyan infants
- PMID: 25420455
- PMCID: PMC6860217
- DOI: 10.1111/mcn.12163
In-home fortification with 2.5 mg iron as NaFeEDTA does not reduce anaemia but increases weight gain: a randomised controlled trial in Kenyan infants
Abstract
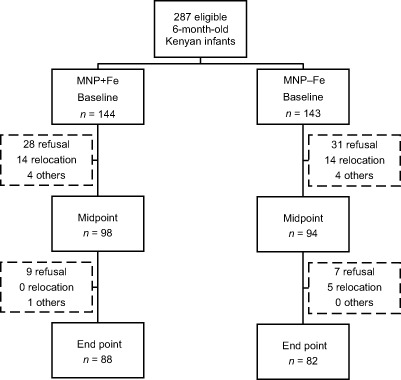
In-home fortification of infants with micronutrient powders (MNPs) containing 12.5 mg iron may increase morbidity from infections; therefore, an efficacious low-dose iron-containing MNP might be advantageous. Effects of iron-containing MNPs on infant growth are unclear. We assessed the efficacy of a low-iron MNP on iron status and growth and monitored safety in a randomised, controlled, double-blind 1-year trial in 6-month-old infants (n = 287) consuming daily a maize porridge fortified with either a MNP including 2.5 mg iron as NaFeEDTA (MNP + Fe) or the same MNP without iron (MNP - Fe). At baseline, after 6 and 12 months, we determined haemoglobin (Hb), iron status [serum ferritin (SF), soluble transferrin receptor (sTfR) and zinc protoporphyrin (ZPP)], inflammation [C-reactive protein (CRP)] and anthropometrics. We investigated safety using weekly morbidity questionnaires asking for diarrhoea, cough, flu, bloody or mucus-containing stool and dyspnoea, and recorded any other illness. Furthermore, feeding history and compliance were assessed weekly. At baseline, 71% of the infants were anaemic and 22% iron deficient; prevalence of inflammation was high (31% had an elevated CRP). Over the 1 year, Hb increased and SF decreased in both groups, without significant treatment effects of the iron fortification. At end point, the weight of infants consuming MNP + Fe was greater than in the MNP - Fe group (9.9 vs. 9.5 kg, P = 0.038). Mothers of infants in the MNP + Fe group reported more infant days spent with cough (P = 0.003) and dyspnoea (P = 0.0002); there were no significant differences on any other of the weekly morbidity measures. In this study, low-dose iron-containing MNP did not improve infant's iron status or reduce anaemia prevalence, likely because absorption was inadequate due to the high prevalence of infections and the low-iron dose.
Keywords: anaemia; growth; infant; iron fortification; micronutrient powder; sub-Saharan Africa.
© 2014 John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

References
-
- Adu‐Afarwuah S., Lartey A., Brown K.H., Zlotkin S., Briend A. & Dewey K.G. (2008) Home fortification of complementary foods with micronutrient supplements is well accepted and has positive effects on infant iron status in Ghana. The American Journal of Clinical Nutrition 87, 929–938. - PubMed
-
- Andang'o P.E., Osendarp S.J., Ayah R., West C.E., Mwaniki D.L., De Wolf C.A. et al (2007) Efficacy of iron‐fortified whole maize flour on iron status of schoolchildren in Kenya: a randomised controlled trial. Lancet 369, 1799–1806. - PubMed
-
- Brown K.H., Peerson J.M., Baker S.K. & Hess S.Y. (2009) Preventive zinc supplementation among infants, preschoolers, and older prepubertal children. Food and Nutrition Bulletin 30, S12–S40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
