

Does low diastolic blood pressure contribute to the risk of recurrent hypertensive cardiovascular disease events? The Framingham Heart Study
- PMID: 25421982
- PMCID: PMC8375430
- DOI: 10.1161/HYPERTENSIONAHA.114.04581
Does low diastolic blood pressure contribute to the risk of recurrent hypertensive cardiovascular disease events? The Framingham Heart Study
Abstract
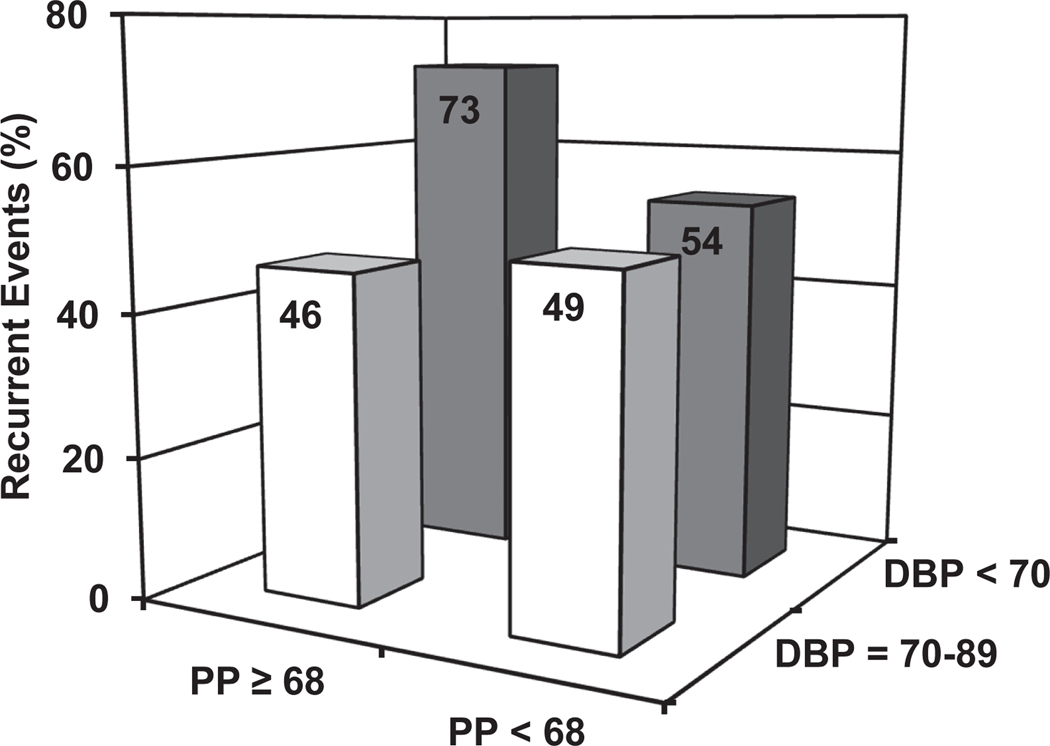
Whether low diastolic blood pressure (DBP) is a risk factor for recurrent cardiovascular disease (CVD) events in persons with isolated systolic hypertension is controversial. We studied 791 individuals (mean age 75 years, 47% female, mean follow-up time: 8±6 years) with DBP <70 (n=225) versus 70 to 89 mm Hg (n=566) after initial CVD events in the original and offspring cohorts of the Framingham Heart Study. Recurrent CVD events occurred in 153 (68%) participants with lower DBP and 271 (48%) with higher DBP (P<0.0001). Risk of recurrent CVD events in risk factor-adjusted Cox regression was higher in those with DBP <70 mm Hg versus DBP 70 to 89 mm Hg in both treated (hazard ratio, 5.1 [95% confidence interval: 3.8-6.9] P<0.0001) and untreated individuals (hazard ratio, 11.7 [95% confidence interval: 6.5-21.1] P<0.0001; treatment interaction: P=0.71). Individually, coronary heart disease, heart failure, and stroke recurrent events were more likely with DBP <70 mm Hg versus 70 to 89 mm Hg (P<0.0001). To examine for an effect of wide pulse pressure on excess risk associated with low DBP, we defined 4 binary groupings of pulse pressure (≥68 versus <68 mm Hg) and DBP (<70 versus 70-89 mm Hg). CVD incidence rates were higher only in the group with pulse pressure ≥68 and DBP <70 mm Hg (76% versus 46%-54%; P<0.001). Persons with isolated systolic hypertension and prior CVD events have increased risk for recurrent CVD events in the presence of DBP <70 mm Hg versus DBP 70 to 89 mm Hg, whether treated or untreated, supporting wide pulse pressure as an important risk modifier for the adverse effect of low DBP.
Keywords: blood pressure; cardiovascular disease; epidemiology.
© 2014 American Heart Association, Inc.
Figures


References
-
- Stewart IMG. Relation of reduction in pressure to first myocardial infarction in patients receiving treatment for severe hypertension. Lance.t 1979;1:861–865. - PubMed
-
- Cruickshank JM, Thorp JM Zacharias FJ. Benefits and potential harm of lowering high blood pressure. Lancet. 1987;1:581–584. - PubMed
-
- Franklin SS, Gustin W, Wong ND, Larson MG, Weber MA, Kannel WB, Levy D. Hemodynamic patterns of age-related changes in blood pressure: the Framingham Heart study. Circulation. 1997;96:308–315. - PubMed
-
- Benetos A, Safar M, Rudnichi A, Smulyan H, Richard JL, Ducimetiere P, Guize L. Pulse pressure: a predictor of long-term cardiovascular mortality in a French male population. Hypertension. 1997;30:1410–1415. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
