

The high-dose aldesleukin "select" trial: a trial to prospectively validate predictive models of response to treatment in patients with metastatic renal cell carcinoma
- PMID: 25424850
- PMCID: PMC4315731
- DOI: 10.1158/1078-0432.CCR-14-1520
The high-dose aldesleukin "select" trial: a trial to prospectively validate predictive models of response to treatment in patients with metastatic renal cell carcinoma
Abstract
Purpose: High-dose aldesleukin (HD IL2) received FDA approval for the treatment of metastatic renal cell carcinoma (MRCC) in 1992, producing a 14% objective response rate (ORR) and durable remissions. Retrospective studies suggested that clinical and pathologic features could predict for benefit. The Cytokine Working Group conducted this prospective trial to validate proposed predictive markers of response to HD IL2.
Experimental design: Standard HD IL2 was administered to prospectively evaluate whether the ORR of patients with mRCC with "good" predictive pathologic features based on an "integrated selection" model [ISM (e.g., clear-cell histology subclassification and carbonic anhydrase-9 (CA-9) IHC staining] was significantly higher than the ORR of a historical, unselected population. Archived tumor was collected for pathologic analysis including tumor programmed death-ligand 1 (PD-L1) expression.
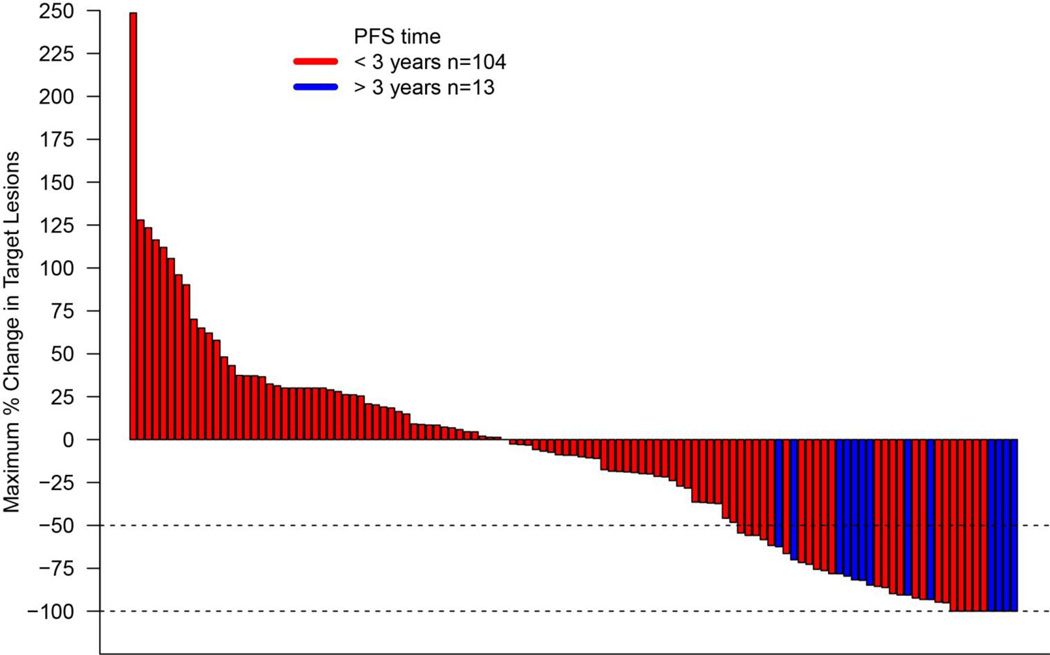
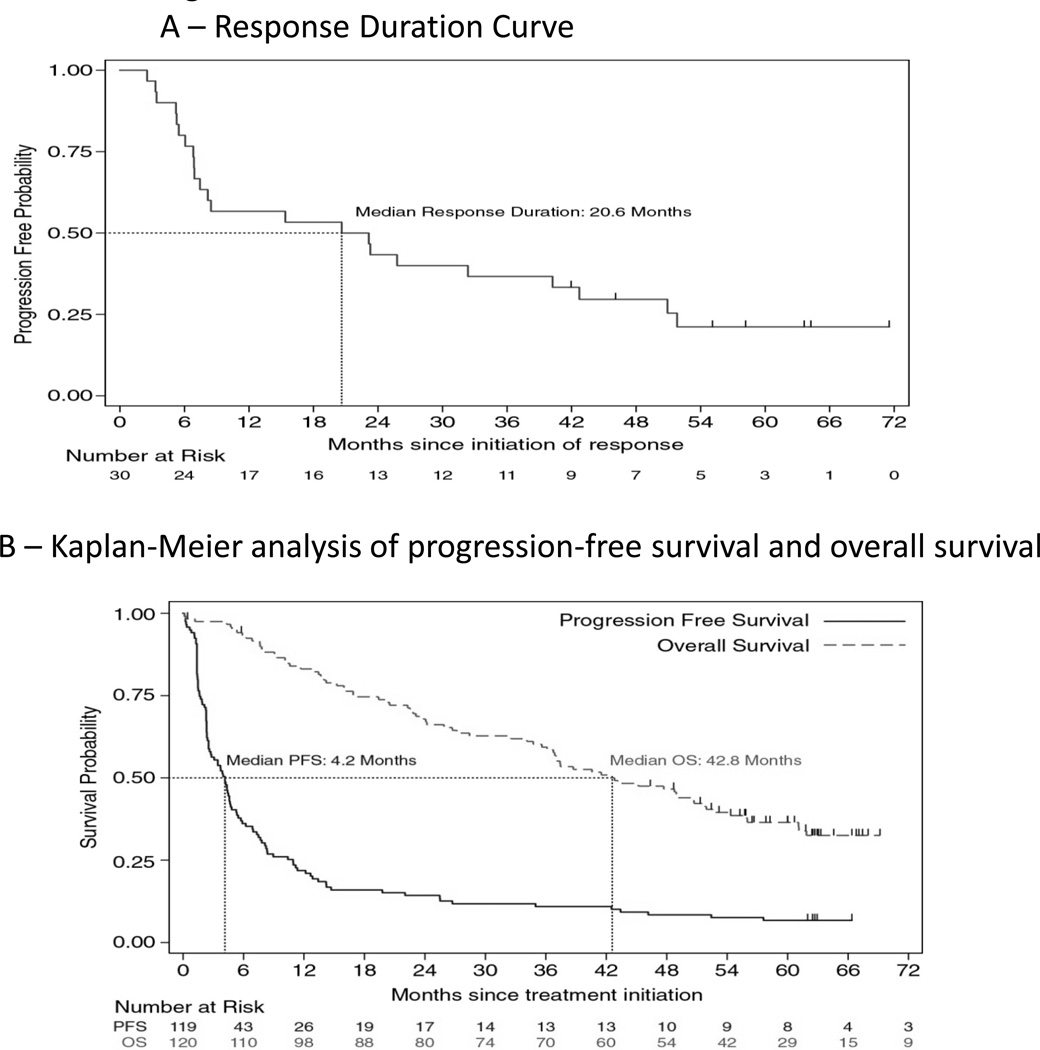
Results: One hundred and twenty eligible patients were enrolled between June 11 and September 7; 70% were Memorial Sloan Kettering Cancer Center (New York, NY) intermediate risk, 96% had clear cell RCC, and 99% had prior nephrectomy. The independently assessed ORR was 25% (30/120, 95% CI, 17.5%-33.7%, P = 0.0014; 3 complete responses, 27 partial responses) and was higher than a historical ORR. Thirteen patients (11%) remained progression free at 3 years and the median overall survival was 42.8 months. ORR was not statistically different by ISM classification ("good-risk" 23% vs. "poor-risk" 30%; P = 0.39). ORR was positively associated with tumor PD-L1 expression (P = 0.01) by IHC.
Conclusions: In this prospective, biomarker validation study, HD IL2 produced durable remissions and prolonged survival in both "good" and "poor-risk" patients. The proposed ISM was unable to improve the selection criteria. Novel markers (e.g., tumor PD L1 expression) appeared useful, but require independent validation.
©2014 American Association for Cancer Research.
Conflict of interest statement
Authors Disclosures of Potential Conflicts of Interest:
Figures
References
-
- Fyfe G, Fisher RI, Rosenberg SA, Sznol M, Parkinson DR, Louie AC. Results of treatment of 255 patients with metastatic renal cell carcinoma who received high-dose recombinant interleukin-2 therapy. J Clin Oncol. 1995;13:688–696. - PubMed
-
- McDermott DF, Regan MM, Clark JI, Flaherty LE, Weiss GR, Logan TF, et al. Randomized phase III trial of high-dose interleukin-2 versus subcutaneous interleukin-2 and interferon in patients with metastatic renal cell carcinoma. J Clin Oncol. 2005;23:133–141. - PubMed
-
- Margolin KA, Rayner AA, Hawkins MJ, Atkins MB, Dutcher JP, Fisher RI, et al. Interleukin-2 and lymphokine-activated killer cell therapy of solid tumors: analysis of toxicity and management guidelines. J Clin Oncol. 1989;7:486–498. - PubMed
-
- Negrier S, Perol D, Ravaud A, Chevreau C, Bay JO, Delva R, et al. Medroxyprogesterone, interferon alfa-2a, interleukin 2, or combination of both cytokines in patients with metastatic renal carcinoma of intermediate prognosis: results of a randomized controlled trial. Cancer. 2007;110:2468–2477. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
