

Initial combination therapy with metformin, pioglitazone and exenatide is more effective than sequential add-on therapy in subjects with new-onset diabetes. Results from the Efficacy and Durability of Initial Combination Therapy for Type 2 Diabetes (EDICT): a randomized trial
- PMID: 25425451
- PMCID: PMC5577982
- DOI: 10.1111/dom.12417
Initial combination therapy with metformin, pioglitazone and exenatide is more effective than sequential add-on therapy in subjects with new-onset diabetes. Results from the Efficacy and Durability of Initial Combination Therapy for Type 2 Diabetes (EDICT): a randomized trial
Abstract
Aim: To test our hypothesis that initiating therapy with a combination of agents known to improve insulin secretion and insulin sensitivity in subjects with new-onset diabetes would produce greater, more durable reduction in glycated haemoglobin (HbA1c) levels, while avoiding hypoglycaemia and weight gain, compared with sequential addition of agents that lower plasma glucose but do not correct established pathophysiological abnormalities.
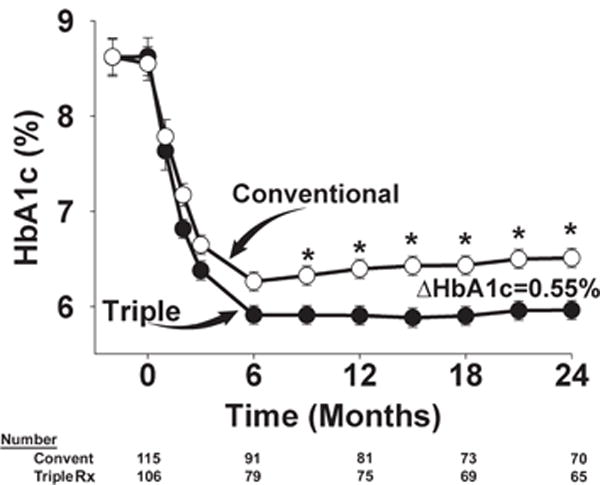
Methods: Drug-naïve, recently diagnosed subjects with type 2 diabetes mellitus (T2DM) were randomized in an open-fashion design in a single-centre study to metformin/pioglitazone/exenatide (triple therapy; n = 106) or an escalating dose of metformin followed by sequential addition of sulfonylurea and glargine insulin (conventional therapy; n = 115) to maintain HbA1c levels at <6.5% for 2 years.
Results: Participants receiving triple therapy experienced a significantly greater reduction in HbA1c level than those receiving conventional therapy (5.95 vs. 6.50%; p < 0.001). Despite lower HbA1c values, participants receiving triple therapy experienced a 7.5-fold lower rate of hypoglycaemia compared with participants receiving conventional therapy. Participants receiving triple therapy experienced a mean weight loss of 1.2 kg versus a mean weight gain of 4.1 kg (p < 0.01) in those receiving conventional therapy.
Conclusion: The results of this exploratory study show that combination therapy with metformin/pioglitazone/exenatide in patients with newly diagnosed T2DM is more effective and results in fewer hypoglycaemic events than sequential add-on therapy with metformin, sulfonylurea and then basal insulin.
Keywords: combination therapy; conventional therapy; durability; glycaemic control.
© 2014 John Wiley & Sons Ltd.
Figures


References
-
- The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–986. - PubMed
-
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352:837–853. - PubMed
-
- Nakagami T, Kawahara R, Hori S, Omori Y. Glycemic control and prevention of retinopathy in Japanese NIDDM patients. A 10-year follow-up study. Diabetes Care. 1997;20:621–622. - PubMed
-
- Klein R, Klein BE, Moss SE. Relation of glycemic control to diabetic microvascular complications in diabetes mellitus. Ann Intern Med. 1996;124:90–96. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
