

Prevalence and variation of Chronic Kidney Disease in the Irish health system: initial findings from the National Kidney Disease Surveillance Programme
- PMID: 25425510
- PMCID: PMC4258258
- DOI: 10.1186/1471-2369-15-185
Prevalence and variation of Chronic Kidney Disease in the Irish health system: initial findings from the National Kidney Disease Surveillance Programme
Abstract
Background: Chronic Kidney Disease (CKD) is a major non-communicable chronic disease that is associated with adverse clinical and economic outcomes. Passive surveillance systems are likely to improve efforts for prevention of chronic kidney disease (CKD) and inform national service planning. This study was conducted to determine the overall prevalence of CKD in the Irish health system, assess period trends and explore patterns of variation as part of a novel surveillance initiative.
Methods: We identified 207, 336 adult patients, age 18 and over, with serum creatinine measurements recorded from a provincial database between 2005-2011 in the Northwest of Ireland. Estimated glomerular filtration rates (eGFR) were determined using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation from standardized creatinine measurements and the presence of CKD was defined as eGFR<60 ml/min per 1.73 m2. Age and sex-specific prevalence estimates were determined for each group while generalized estimating equations (GEE) and multivariable logistic regression were used to explore associations using adjusted odds ratios (AOR) and 95% confidence intervals (95% CI).
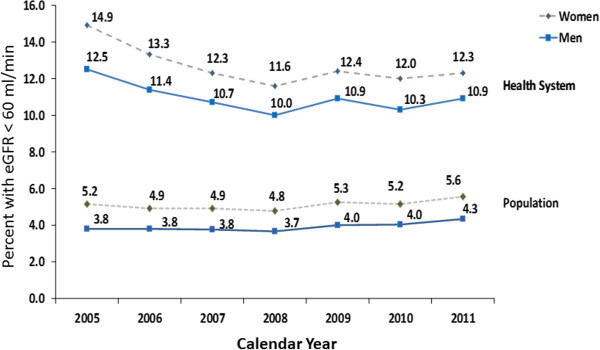
Results: The prevalence of CKD in the health system was 11.8% (95% CI 11.8-12.1); 10.9% in men (10.7-11.1) and 12.6% in women (12.4-12.8). This corresponded to a detection rate of 4.5% (5.1% in women and 3.9% in men). The prevalence of CKD was significantly higher in women than in men (12.6% versus 10.9%, P<0.001), older age groups, and among patients with a history of Acute Kidney Injury (AKI) than without (45.2% versus 10.7%, P<0.0001). Multivariable analysis identified advancing age, female gender, location of medical supervision, county of residence, and AKI as significant determinants of prevalence.
Conclusion: The prevalence of CKD in the Irish health system is 11.8% corresponding to a detection rate of 4.5% in the general population. Demographic, geographic factors and acute kidney injury episodes are important determinants of disease burden. Passive surveillance of CKD is both feasible and desirable within the Irish health system, and offers huge opportunities for targeted prevention programmes and improved clinical outcomes.
Figures

References
-
- Ayodele OE, Alebiosu CO. Burden of chronic kidney disease: an international perspective. ACKD. 2010;17:215–224. - PubMed
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2369/15/185/prepub
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
