

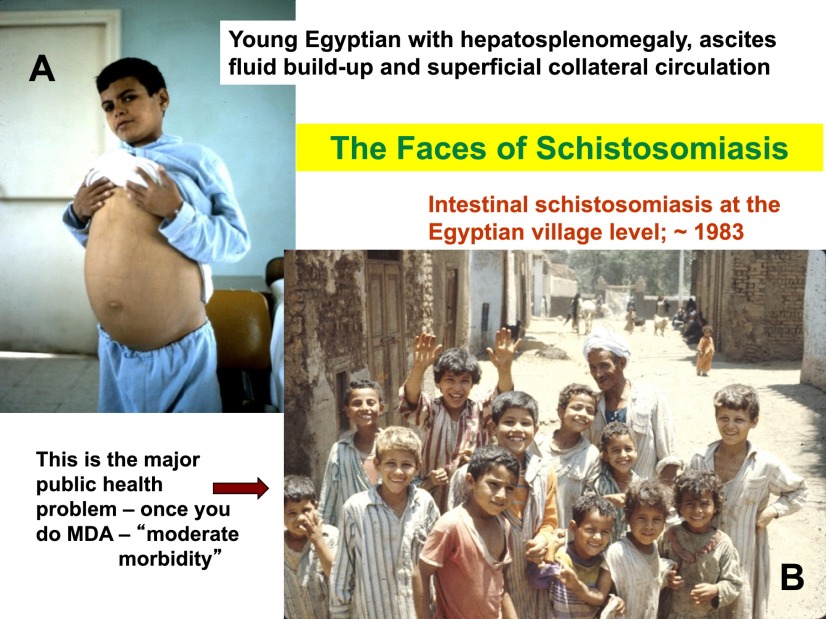
Morbidity control of schistosomiasis by mass drug administration: how can we do it best and what will it take to move on to elimination?
- PMID: 25425948
- PMCID: PMC4204048
- DOI: 10.2149/tmh.2014-S04
Morbidity control of schistosomiasis by mass drug administration: how can we do it best and what will it take to move on to elimination?
Abstract
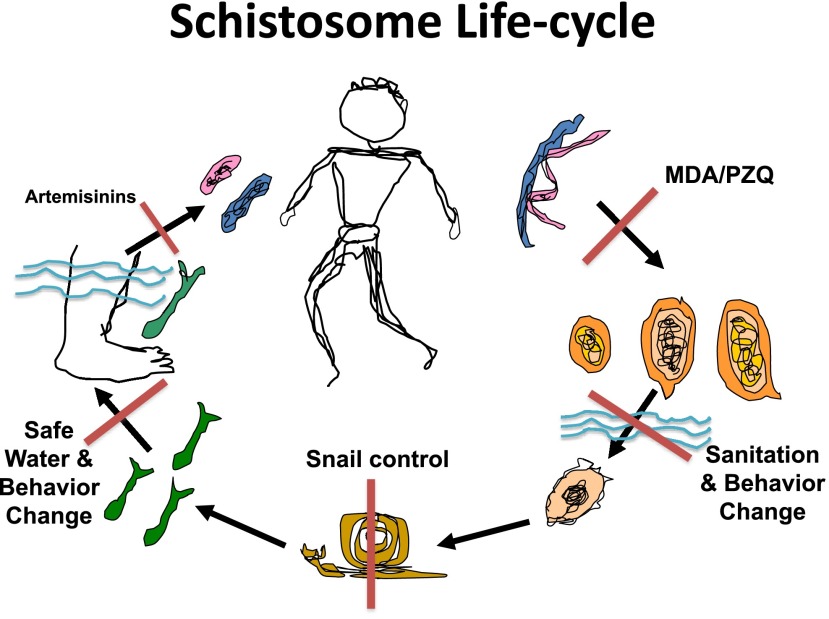
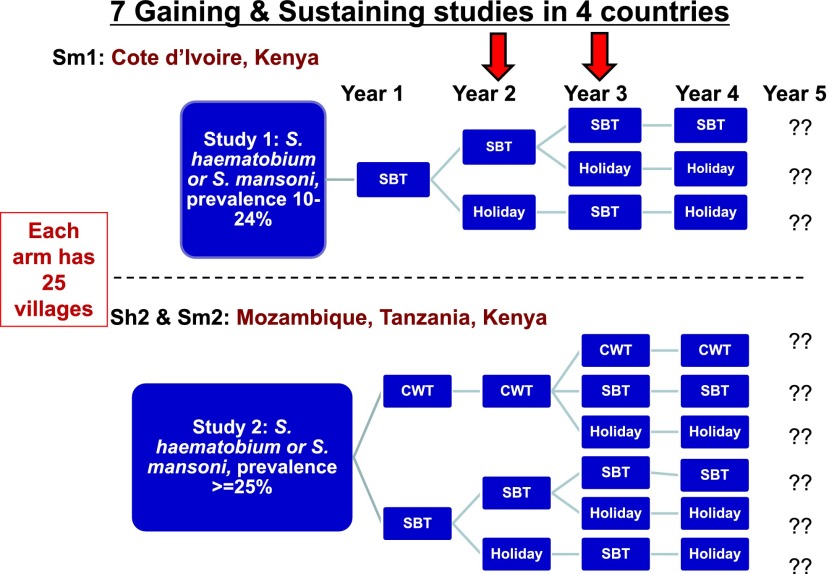
The World Health Organization (WHO) has, for some time, encouraged countries endemic for schistosomiasis to control morbidity from this disease through mass drug administration (MDA) of the well-tolerated drug, praziquantel (PZQ). With the London Declaration in January 2012 and the promise by Merck Serono to eventually donate 250 million PZQ tablets per year, most endemic countries in sub-Saharan Africa have now developed national plans to do MDA for schistosomiasis morbidity control. More recently, based on two World Health Assembly (WHA) resolutions (WHA 54.19 & WHA 65.21) on schistosomiasis, countries are further encouraged to eliminate schistosomiasis, where feasible. The fight against schistosomiasis is therefore in a critical period of tremendous opportunities and equal challenges. How do we do the most effective job of MDA? What tools do we need to do this job better? How will we know when to move from morbidity control to elimination? What combinations of interventions, beyond MDA, are needed to eliminate transmission? The Schistosomiasis Consortium for Operational Research and Evaluation (SCORE) has its Secretariat at the University of Georgia and with programs in more than 26 institutions in 19 countries it is trying to answer these very practical questions through multiple large field-based studies and the evaluation or development of better diagnostics for schistosomiasis. This presentation will summarize the current status of morbidity control and elimination programs and the operational research by SCORE that we hope will provide much-needed answers for national program managers so they can most effectively pursue these critical public health programs.
Keywords: Control; Diagnostics; Elimination; Mass Drug Administration; Operational Research; Schistosomiasis.
Figures

References
-
- King CH, Dickman K, Tisch DJ. Reassessment of the cost of chronic helminthic infection: a meta-analysis of disability-related outcomes in endemic schistosomiasis. Lancet 2005; 365(9470): 1561–1569. - PubMed
-
- Ezeamam AE, McGarvey ST, Hogan J, Lapane KL, Bellinger DC, Acosta LP, Leenstra T, Oveda RM, Kurtis JD, Friedman JF. Treatment for Schistosoma japonicum, reduction of intestinal parasite load, and cognitive test score improvements in school-aged children. PLoS Negl Trop Dis 2012; 6(5): e1634. - PMC - PubMed
-
- Friedman JF, Kanzaria HK, McGarvey ST. Human schistosomiasis and anemia: the relationship and potential mechanisms. Trends Parasitol 2005; 21(8): 386–392. - PubMed
-
- Savioli L, Hatz C, Dixon H, Kisumku UM, Mott KE. Control of morbidity due to Schistosoma haematobium on Pemba Island: egg excretion and hematuria as indicators of infection. Am J Trop Med Hyg 1990; 43(3): 289–295. - PubMed
-
- WHO. Preventive Chemotherapy in Human Helminthiasis: Coordinated Use of Antihelminthic Drugs in Control Interventions: A Manual for Health Professionals and Programme Managers. Geneva: World Health Organization; 2006.
LinkOut - more resources
Full Text Sources
Other Literature Sources