

Intravenous leiomyomatosis with intracardiac extension: echocardiographic study and literature review
- PMID: 25425982
- PMCID: PMC4189351
- DOI: 10.14503/THIJ-13-3533
Intravenous leiomyomatosis with intracardiac extension: echocardiographic study and literature review
Abstract
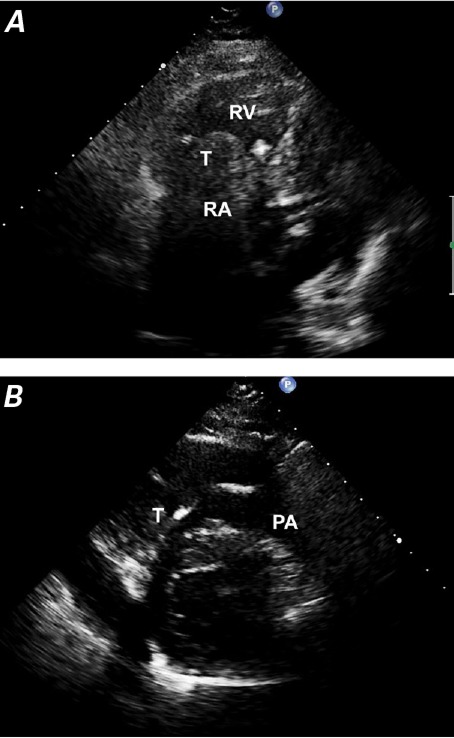
Uterine leiomyomatosis is a common disease in women; however, intravenous leiomyomatosis with intracaval and intracardiac tumor extension is rare. We sought to analyze the clinical and echocardiographic features of intracardiac leiomyomatosis. From January 2003 through July 2012, 7 women (age range, 24-59 yr) underwent surgical resection of histopathologically diagnosed intracardiac leiomyomas at our hospital. Most of the patients had histories of hysterectomy or uterine leiomyoma. We retrospectively analyzed their preoperative echocardiograms. We found that the tumors had no stalks, did not adhere to the wall of the right side of the heart, were highly mobile, and moved back and forth in the right atrium near the tricuspid orifice. All tumors originated from the inferior vena cava and had borders well demarcated from that structure's wall. Most of the masses extended into the inferior vena cava and right atrium through the right internal and common iliac veins. Computed tomograms revealed pelvic tumors and contiguous filling defects in 6 patients. When echocardiograms reveal a right-sided cardiac mass that originates from the inferior vena cava, particularly in women who have a history of hysterectomy or uterine leiomyoma, intracardiac leiomyomatosis should be suspected. If the mass has no stalk and freely moves within the inferior vena cava and right-sided cardiac chambers without attachment to the endothelial surface or endocardium, intracardiac leiomyomatosis should be diagnosed. We discuss our findings and briefly review the relevant medical literature.
Keywords: Diagnosis, differential; diagnostic imaging/methods; heart neoplasms/pathology/secondary/surgery; leiomyoma/diagnosis/ultrastructure; leiomyomatosis/complications/pathology; neoplasm invasiveness; uterine neoplasms/pathology/ultrastructure; vena cava, inferior/pathology.
Figures





References
-
- Clement PB. Intravenous leiomyomatosis of the uterus. Pathol Annu. 1988;23(Pt 2):153–83. - PubMed
-
- Lam PM, Lo KW, Yu MY, Wong WS, Lau JY, Arifi AA, Cheung TH. Intravenous leiomyomatosis: two cases with different routes of tumor extension. J Vasc Surg. 2004;39(2):465–9. - PubMed
-
- Castelli P, Caronno R, Piffaretti G, Tozzi M. Intravenous uterine leiomyomatosis with right heart extension: successful two-stage surgical removal. Ann Vasc Surg. 2006;20(3):405–7. - PubMed
-
- Mulvany NJ, Slavin JL, Ostor AG, Fortune DW. Intravenous leiomyomatosis of the uterus: a clinicopathologic study of 22 cases. Int J Gynecol Pathol. 1994;13(1):1–9. - PubMed
-
- Baca Lopez FM, Martinez-Enriquez A, Castrejon-Aivar FJ, Ruanova-Leon D, Yanez-Gutierrez L. Echocardiographic study of an intravenous leiomyoma: case report and review of the literature. Echocardiography. 2003;20(8):723–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
