

Beta-blockers reduced the risk of mortality and exacerbation in patients with COPD: a meta-analysis of observational studies
- PMID: 25427000
- PMCID: PMC4245088
- DOI: 10.1371/journal.pone.0113048
Beta-blockers reduced the risk of mortality and exacerbation in patients with COPD: a meta-analysis of observational studies
Abstract
Background: Cardiovascular disease is a primary cause of death in patients with chronic obstructive pulmonary disease (COPD). Beta-blockers have been proved to reduce morbidity and improve survival in patients with cardiac diseases. But the effects of beta-blockers on outcomes in patients with COPD remain controversial. The objective of this meta-analysis was to assess the effect of beta-blockers on mortality and exacerbation in patients with COPD.
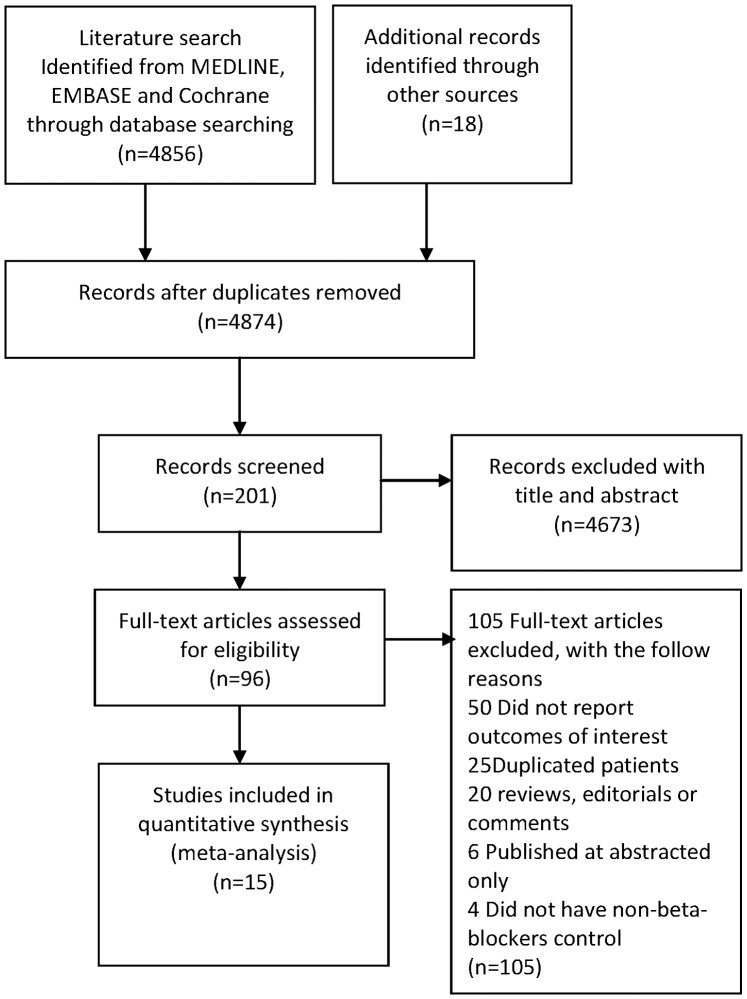
Methods: An extensive search of the EMBASE, MEDLINE and Cochrane was performed to retrieve the studies of beta-blockers treatment in patients with COPD. The random effects model meta-analysis was used to evaluate effect on overall mortality and exacerbation of COPD.
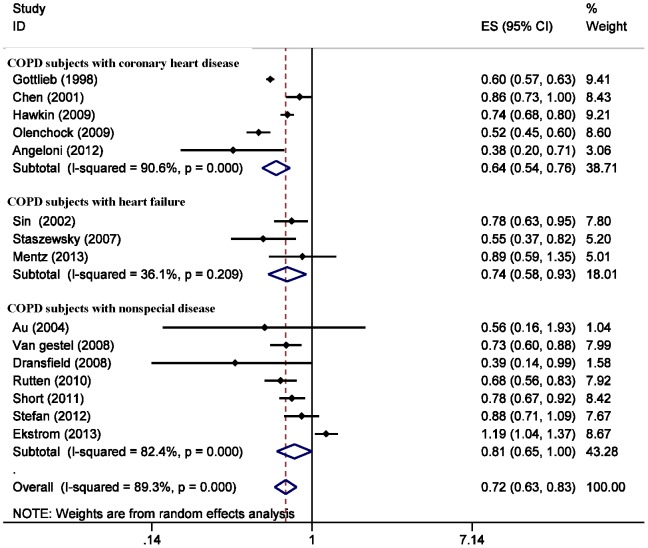
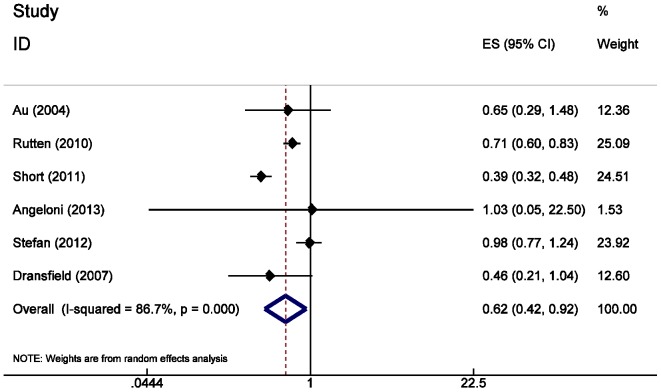
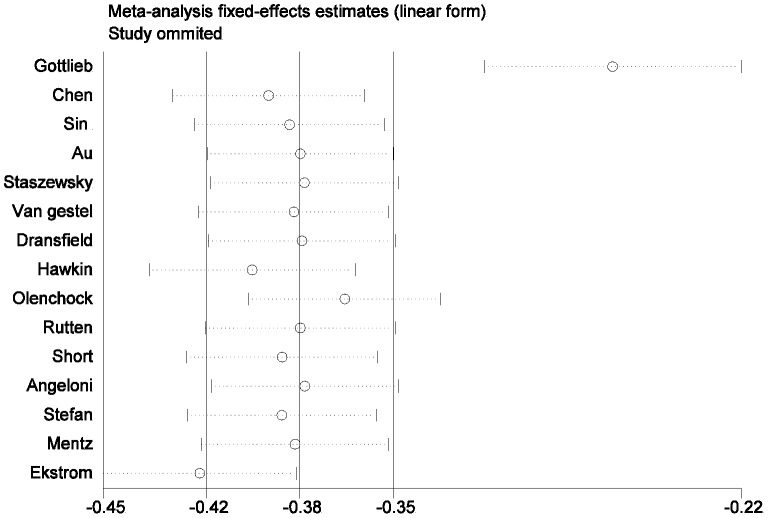
Results: Fifteen original observational cohort studies with a follow-up time from 1 to 7.2 years were included. The results revealed that beta-blockers treatment significantly decreased the risk of overall mortality and exacerbation of COPD. The relative risk (RR) for overall mortality was 0.72 (0.63 to 0.83), and for exacerbation of COPD was 0.63 (0.57 to 0.71). In subgroup analysis of COPD patients with coronary heart disease or heart failure, the risk for overall mortality was 0.64 (0.54-0.76) and 0.74 (0.58-0.93), respectively.
Conclusion: The findings of this meta-analysis confirmed that beta-blocker use in patients with COPD may not only decrease the risk of overall mortality but also reduce the risk of exacerbation of COPD. Beta-blocker prescription for cardiovascular diseases needs to improve in COPD patients.
Conflict of interest statement
Figures
References
-
- Chapman KR, Mannino DM, Soriano JB, Vermeire PA, Buist AS, et al.. (2006) Epidemiology and costs of chronic obstructive pulmonary disease. European Respiratory Journal 27(1):: 188–207. - PubMed
-
- Kuller LH, Ockene JK, Townsend M, Browner W, Meilahn E, et al. (1989) The epidemiology of pulmonary function and COPD mortality in the multiple risk factor intervention trial. Am Rev Respir Dis 140:S76–S81. - PubMed
-
- Smith SC, Allen J, Blair SN, Bonow RO, Brass LM, et al.. (2006) AHA/ACC Guidelines for Secondary Prevention for Patients With Coronary and Other Atherosclerotic Vascular Disease: 2006 Update Endorsed by the National Heart, Lung, and Blood Institute. Journal of the American College of Cardiology 47(10): 2130–2139. - PubMed
-
- Abraham WT, Chin FMH, Feldman AM, Francis FGS, Ganiats FTG, et al.. (2009) 2009 Focused Update Incorporated Into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults. Journal of the American College of Cardiology 53(15): e1–90. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
