

The role of FDG-PET in defining prognosis of Hodgkin lymphoma for early-stage disease
- PMID: 25428223
- PMCID: PMC4467863
- DOI: 10.1182/blood-2014-05-577627
The role of FDG-PET in defining prognosis of Hodgkin lymphoma for early-stage disease
Erratum in
- Blood. 2015 Apr 9;125(15):2450
Abstract
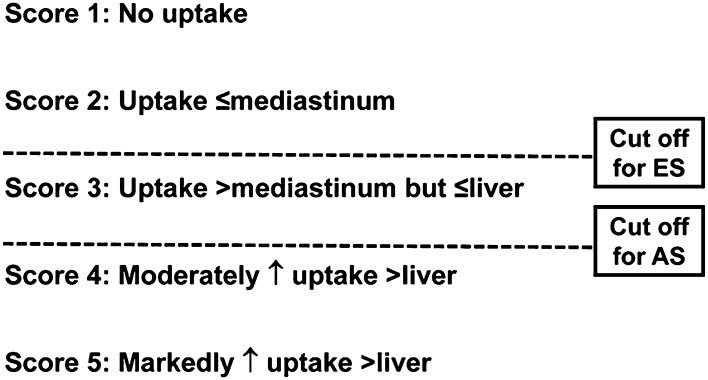
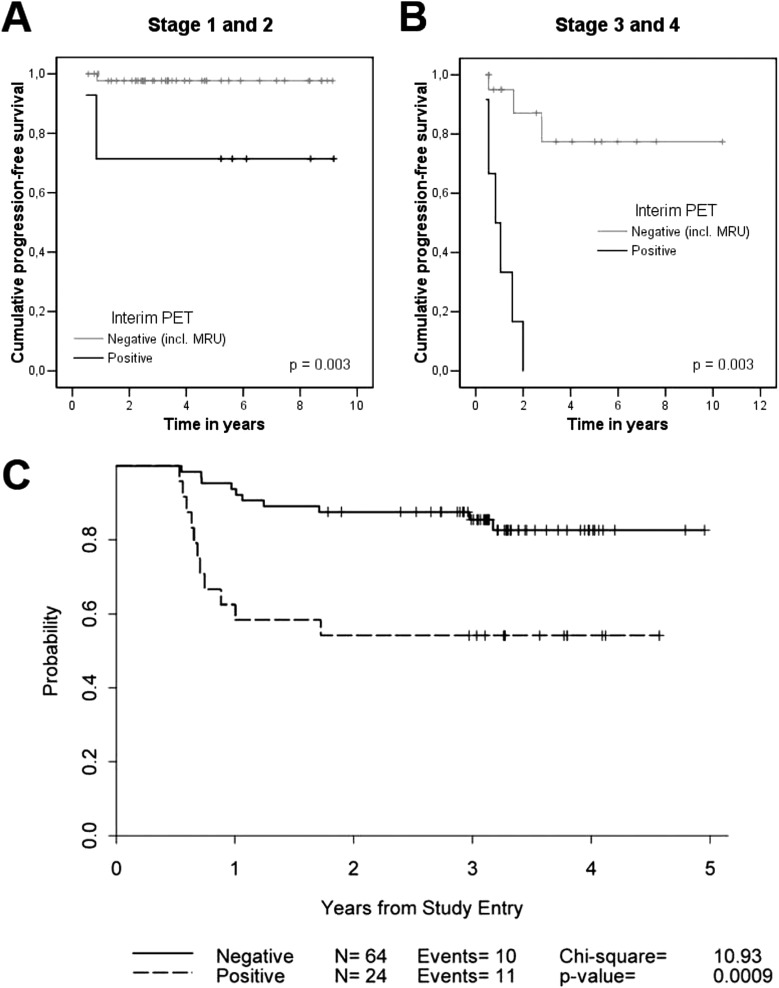
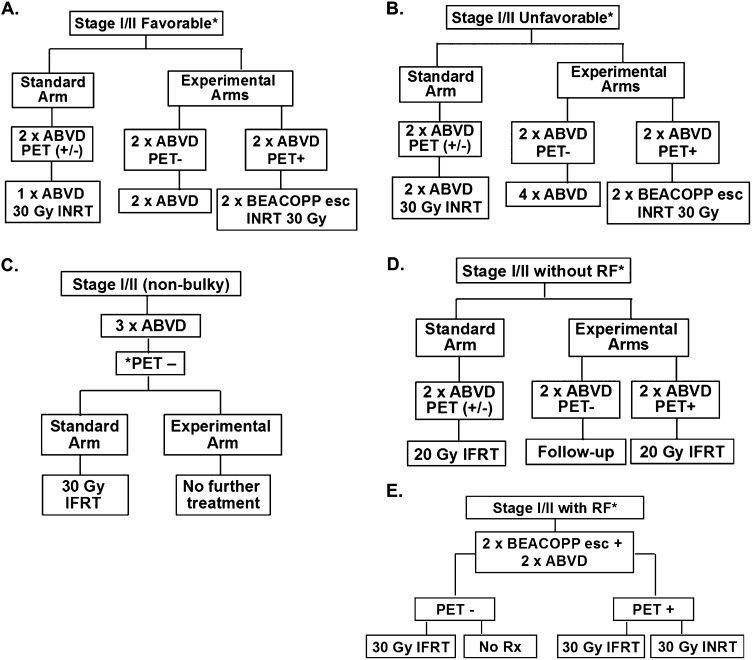
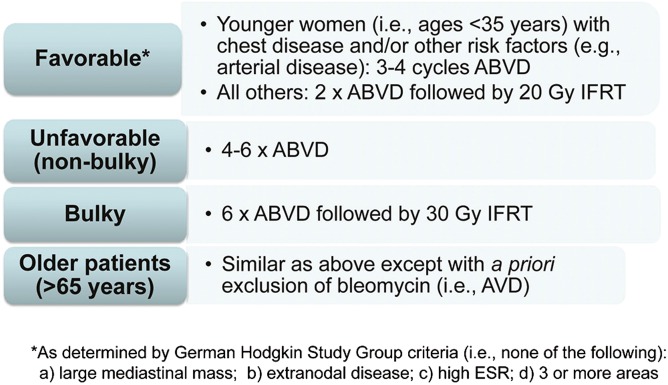
Given the excellent survival rates for early-stage Hodgkin lymphoma (HL), the young age of many patients, and concerns regarding acute and late treatment-related toxicities, there is a desire to have a predictive tool that enables therapy to be tailored toward the individual patient. Early (or interim) (18)F-fluorodeoxyglucose positron emission tomography with computerized tomography (FDG-PET/CT), as a test of tumor sensitivity to ongoing/planned therapy, has been shown to be prognostic for survival in HL. Based on results of interim FDG-PET/CT, therapy may be subsequently modified through minimization or via intensification for low- and high-risk patient populations, respectively (ie, response-adapted therapy). Important data have been generated to standardize the interpretability and reproducibility of interim FDG-PET/CT (eg, the Deauville 5-point system), and observational and noncontrolled prospective studies have produced evidence supporting the hypothesis that response-adapted therapy may potentially serve as a predictive tool. Furthermore, results from noninferiority phase 3 clinical trials randomizing early-stage HL patients with negative interim FDG-PET/CT to combined modality therapy versus chemotherapy alone have been reported. The current collective findings from these randomized early-stage HL studies have shown that acute relapse rates are lower with combined modality therapy, even in patients with negative interim FDG-PET/CT. Additional randomized response-adapted studies are ongoing and novel FDG-PET/CT applications involving quantitative techniques and innovative imaging modalities are being investigated to identify more robust imaging biomarkers. Treatment of early-stage HL remains a clinical management choice for physicians and patients to make with consideration of acute and long-term outcomes.
© 2014 by The American Society of Hematology. All rights reserved.
Figures
References
-
- Canellos GP, Rosenberg SA, Friedberg JW, Lister TA, Devita VT. Treatment of Hodgkin lymphoma: a 50-year perspective. J Clin Oncol. 2014;32(3):163–168. - PubMed
-
- Bartlett NL. Limited-stage Hodgkin lymphoma: optimal chemotherapy and the role of radiotherapy. Am Soc Clin Oncol Educ Book. 2013:374–380. - PubMed
-
- Eichenauer DA, Thielen I, Haverkamp H, et al. Therapy-related acute myeloid leukemia and myelodysplastic syndromes in patients with Hodgkin lymphoma: a report from the German Hodgkin Study Group. Blood. 2014;123(11):1658–1664. - PubMed
-
- Hodgson DC. Late effects in the era of modern therapy for Hodgkin lymphoma. Hematology Am Soc Hematol Educ Program. 2011;2011:323–329. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
