

Pneumonia Pathogen Characterization Is an Independent Determinant of Hospital Readmission
- PMID: 25429607
- PMCID: PMC7127757
- DOI: 10.1378/chest.14-2129
Pneumonia Pathogen Characterization Is an Independent Determinant of Hospital Readmission
Abstract
Background: Hospital readmissions for pneumonia occur often and are difficult to predict. For fiscal year 2013, the Centers for Medicare & Medicaid Services readmission penalties have been applied to acute myocardial infarction, heart failure, and pneumonia. However, the overall impact of pneumonia pathogen characterization on hospital readmission is undefined.
Methods: This was a retrospective 6-year cohort study (August 2007 to September 2013).
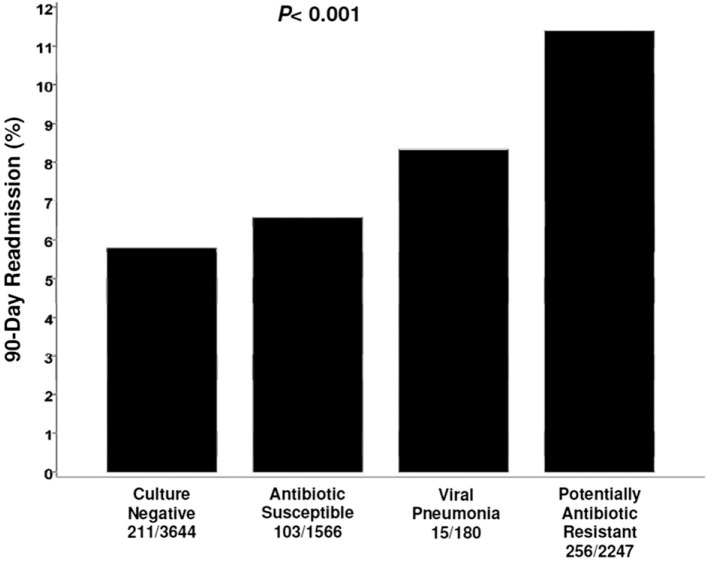
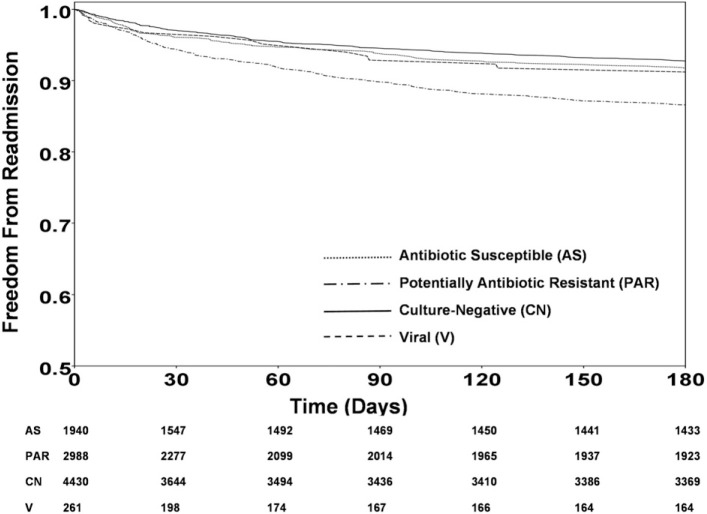
Results: We evaluated 9,624 patients with a discharge diagnosis of pneumonia. Among these patients, 4,432 (46.1%) were classified as having culture-negative pneumonia, 1,940 (20.2%) as having pneumonia caused by antibiotic-susceptible bacteria, 2,991 (31.1%) as having pneumonia caused by potentially antibiotic-resistant bacteria, and 261 (2.7%) as having viral pneumonia. The 90-day hospital readmission rate for survivors (n = 7,637, 79.4%) was greatest for patients with pneumonia attributed to potentially antibiotic-resistant bacteria (11.4%) followed by viral pneumonia (8.3%), pneumonia attributed to antibiotic-susceptible bacteria (6.6%), and culture-negative pneumonia (5.8%) (P < .001). Multiple logistic regression analysis identified pneumonia attributed to potentially antibiotic-resistant bacteria to be independently associated with 90-day readmission (OR, 1.75; 95% CI, 1.56-1.97; P < .001). Other independent predictors of 90-day readmission were Charlson comorbidity score > 4, cirrhosis, and chronic kidney disease. Culture-negative pneumonia was independently associated with lower risk for 90-day readmission.
Conclusions: Readmission after hospitalization for pneumonia is relatively common and is related to pneumonia pathogen characterization. Pneumonia attributed to potentially antibiotic-resistant bacteria is associated with an increased risk for 90-day readmission, whereas culture-negative pneumonia is associated with lower risk for 90-day readmission.
Figures
Comment in
-
Admitting What We Do Not Know About Pneumonia Readmissions.Chest. 2015 Jul;148(1):4-6. doi: 10.1378/chest.14-2987. Chest. 2015. PMID: 26149547 No abstract available.
-
Identifying Pathogen in Culture-Negative Pneumonia.Chest. 2016 Feb;149(2):609-610. doi: 10.1016/j.chest.2015.10.077. Chest. 2016. PMID: 26867850 No abstract available.
References
-
- Marks E. Complexity science and the readmission dilemma. JAMA Intern Med. 2013;173(8):629–631. - PubMed
-
- Medicare Payment Advisory Commission Refining the hospital readmissions reduction program. http://www.medpac.gov/documents/reports/jun13_ch04.pdf?sfvrsn=0 Accessed June 27, 2014.
-
- Fontanarosa PB, McNutt RA. Revisiting hospital readmissions. JAMA. 2013;309:398–400. - PubMed
-
- Kocher RP, Adashi EY. Hospital readmissions and the Affordable Care Act: paying for coordinated quality care. JAMA. 2011;306(16):1794–1795. - PubMed
-
- Hansen LO, Young RS, Hinami K, Leung A, Williams MV. Interventions to reduce 30-day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
