

The utility of cardiac MRI in diagnosis of infective endocarditis: preliminary results
- PMID: 25430531
- PMCID: PMC4463365
- DOI: 10.5152/dir.2014.14239
The utility of cardiac MRI in diagnosis of infective endocarditis: preliminary results
Abstract
Purpose: We aimed to evaluate the utility of cardiac magnetic resonance imaging (MRI) for the diagnosis of infective endocarditis (IE).
Methods: Sixteen patients with a preliminary diagnosis of IE (10 women and six men; age range, 4-66 years) were referred for cardiac MRI. MRI sequences were as follows: echo-planar cine true fast imaging with steady-state precession (true-FISP), dark-blood fast spin echo T1-weighted imaging, T2-weighted imaging, dark-blood half-Fourier single shot turbo spin echo (HASTE), and early contrast-enhanced first-pass fast low-angle shot (FLASH). Delayed contrast-enhanced images were obtained using three-dimensional inversion recovery FLASH after 15±5 min. The MRI features were evaluated, including valvular pathologies on cine MRI and contrast enhancement on the walls of the cardiac chambers, major thoracic vasculature, and paravalvular tissue, attributable to endothelial extension of inflammation on contrast-enhanced images.
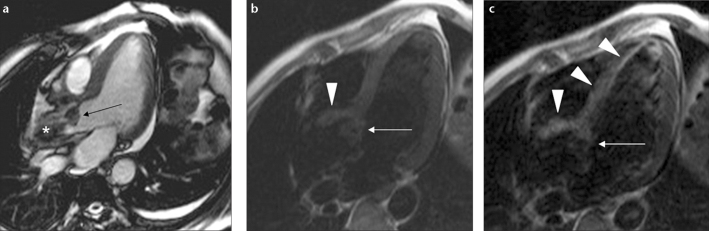
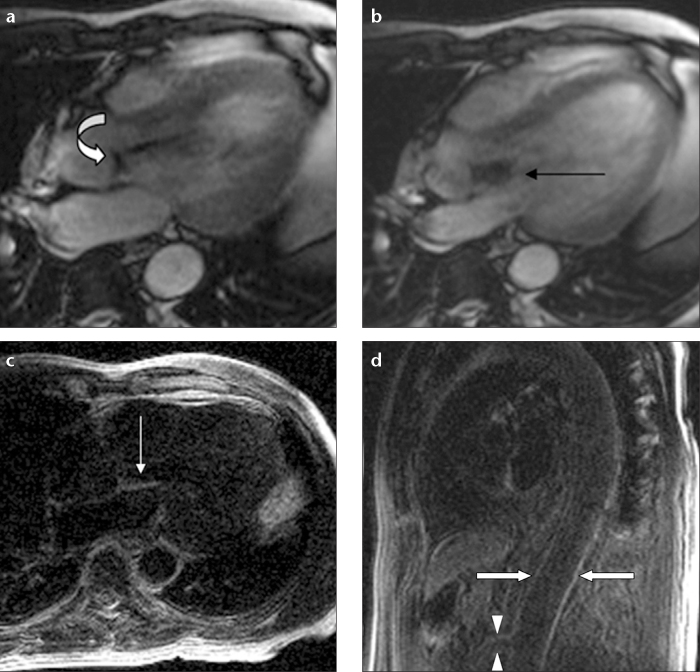
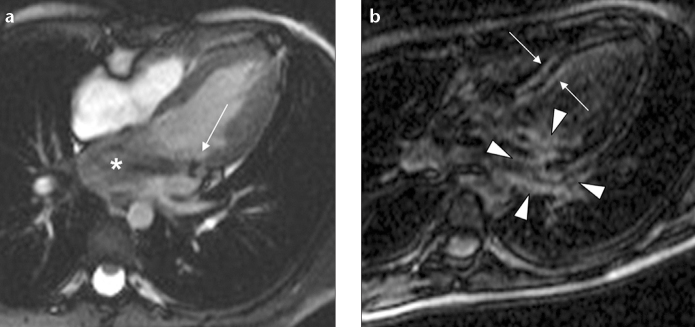
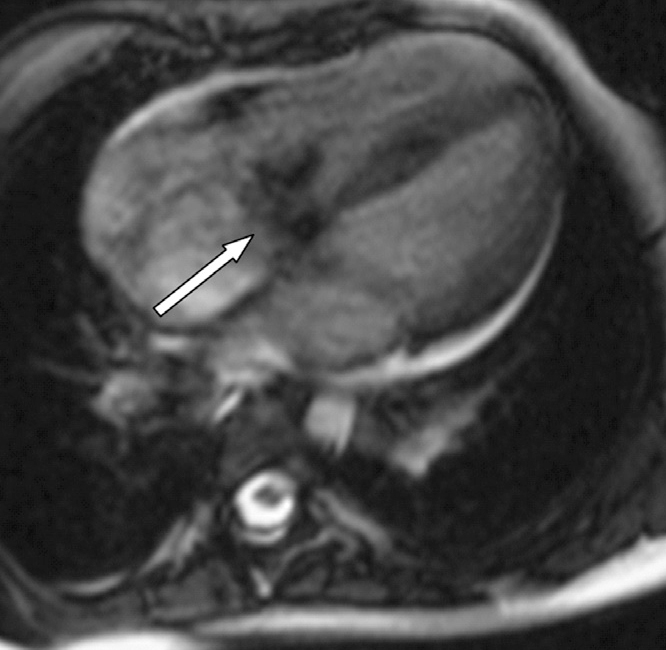
Results: Fourteen valvular vegetations were detected in eleven patients on cardiac MRI. It was not possible to depict valvular vegetations in five patients. Vegetations were detected on the aortic valve (n=7), mitral valve (n=3), tricuspid and pulmonary valves (n=1). Delayed contrast enhancement attributable to extension of inflammation was observed on the aortic wall and aortic root (n=11), paravalvular tissue (n=4), mitral valve (n=2), walls of the cardiac chambers (n=6), interventricular septum (n=3), and wall of the pulmonary artery and superior mesenteric artery (n=1).
Conclusion: Valvular vegetation features of IE can be detected by MRI. Moreover, in the absence of vegetations, detection of delayed enhancement representing endothelial inflammation of the cardiovascular structures can contribute to the diagnosis and treatment planning of IE.
Figures

References
-
- Bashore TM, Cabell C, Fowler V., Jr Update on infective endocarditis. Curr Probl Cardiol. 2006;31:274–352. - PubMed
-
- Karchmer A. Infective endocarditis. In: Zipes DP, Libby P, Bonow RO, editors. Heart Disease. Philadelphia: Elsevier Saunders; 2005. pp. 1633–1656.
-
- Rodbard S. Blood velocity and endocarditis. Circulation. 1963;27:18–28. - PubMed
-
- Todd AJ, Leslie SJ, Macdougall M, Denvir MA. Clinical features remain important for the diagnosis of infective endocarditis in the modern era. QJM. 2006;99:23–31. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
