

Treatment of bloodstream infections in ICUs
- PMID: 25431091
- PMCID: PMC4289315
- DOI: 10.1186/1471-2334-14-489
Treatment of bloodstream infections in ICUs
Abstract
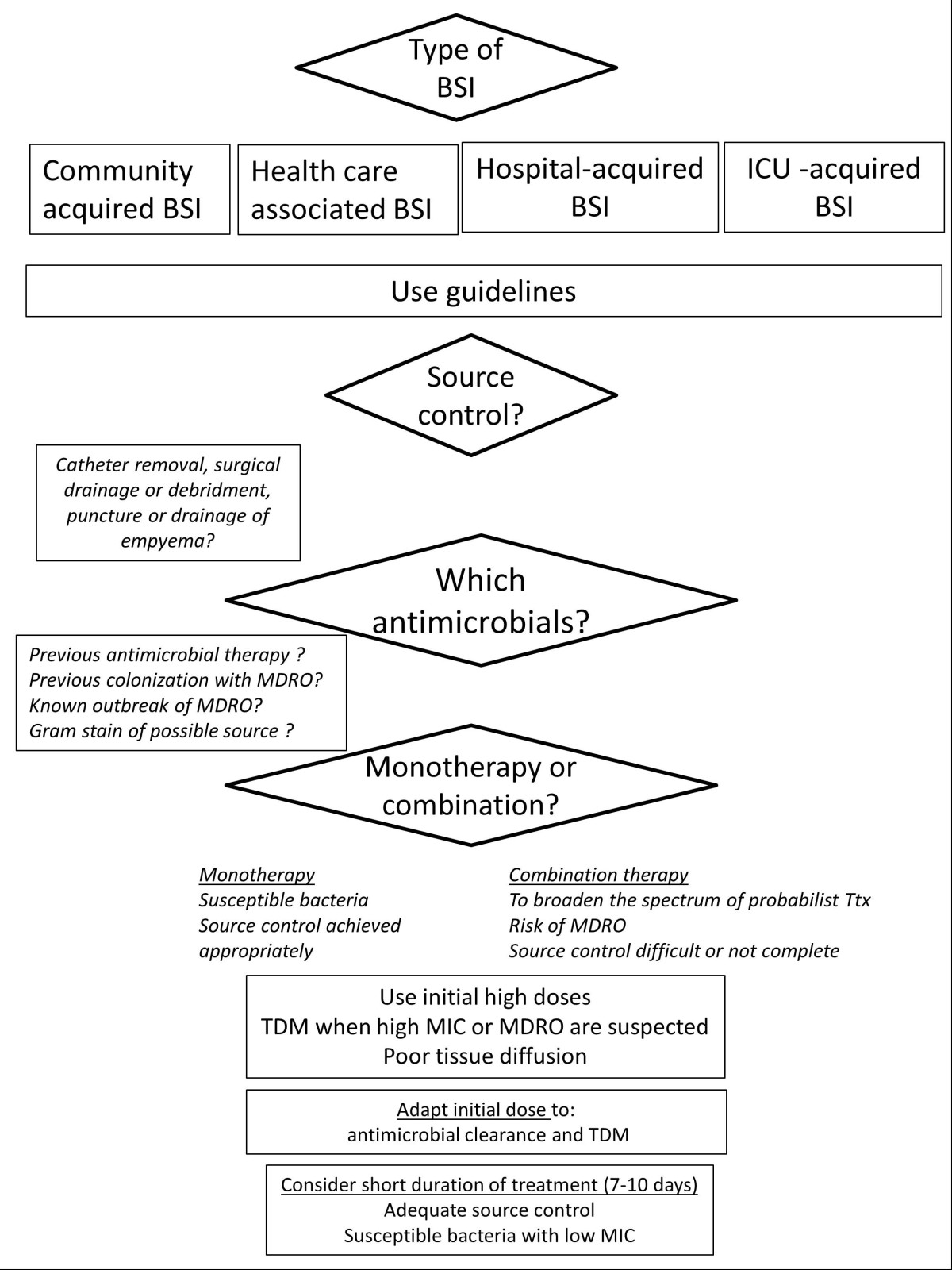
Bloodstream infections (BSIs) are frequent in ICU and is a prognostic factor of severe sepsis. Community acquired BSIs usually due to susceptible bacteria should be clearly differentiated from healthcare associated BSIs frequently due to resistant hospital strains. Early adequate treatment is key and should use guidelines and direct examination of samples performed from the infectious source. Previous antibiotic therapy knowledge, history of multi-drug resistant organism (MDRO) carriage are other major determinants of first choice antimicrobials in heathcare-associated and nosocomial BSIs. Initial antimicrobial dose should be adapted to pharmacokinetic knowledge. In general, a high dose is recommended at the beginning of treatment. If MDRO is suspected combination antibiotic therapy is mandatory because it increase the spectrum of treatment. Most of time, combination should be pursued no more than 2 to 5 days.Given the negative impact of useless antimicrobials, maximal effort should be done to decrease the antibiotic selection pressure. De-escalation from a broad spectrum to a narrow spectrum antimicrobial decreases the antibiotic selection pressure without negative impact on mortality. Duration of therapy should be shortened as often as possible especially when organism is susceptible, when the infection source has been totally controlled.
Figures
Similar articles
-
Bloodstream infections in critically ill patients: an expert statement.Intensive Care Med. 2020 Feb;46(2):266-284. doi: 10.1007/s00134-020-05950-6. Epub 2020 Feb 11. Intensive Care Med. 2020. PMID: 32047941 Free PMC article.
-
Current guidelines for the treatment of severe pneumonia and sepsis.Chemotherapy. 2005 Aug;51(5):227-33. doi: 10.1159/000087452. Chemotherapy. 2005. PMID: 16103664 Review.
-
Antimicrobial consumption, costs and resistance patterns: a two year prospective study in a Romanian intensive care unit.BMC Infect Dis. 2017 May 22;17(1):358. doi: 10.1186/s12879-017-2440-7. BMC Infect Dis. 2017. PMID: 28532467 Free PMC article.
-
Antibiotic strategies in severe nosocomial sepsis: why do we not de-escalate more often?Crit Care Med. 2012 May;40(5):1404-9. doi: 10.1097/CCM.0b013e3182416ecf. Crit Care Med. 2012. PMID: 22430235
-
Surviving Sepsis in the Intensive Care Unit: The Challenge of Antimicrobial Resistance and the Trauma Patient.World J Surg. 2017 May;41(5):1165-1169. doi: 10.1007/s00268-016-3531-0. World J Surg. 2017. PMID: 27146052 Review.
Cited by
-
[Antibiotic stewardship : Measures for optimizing prescription of anti-infective agents].Anaesthesist. 2018 Jan;67(1):3-8. doi: 10.1007/s00101-017-0398-x. Anaesthesist. 2018. PMID: 29313072 Review. German.
-
Heterogeneity in the treatment of bloodstream infections identified from antibiotic exposure mapping.Pharmacoepidemiol Drug Saf. 2019 May;28(5):707-715. doi: 10.1002/pds.4761. Epub 2019 Mar 27. Pharmacoepidemiol Drug Saf. 2019. PMID: 30916833 Free PMC article.
-
Clinical impact and cost-consequence analysis of ePlex® blood culture identification panels for the rapid diagnosis of bloodstream infections: a single-center randomized controlled trial.Eur J Clin Microbiol Infect Dis. 2024 Jun;43(6):1193-1203. doi: 10.1007/s10096-024-04820-z. Epub 2024 Mar 27. Eur J Clin Microbiol Infect Dis. 2024. PMID: 38536524 Free PMC article. Clinical Trial.
-
Biochips for Direct Detection and Identification of Bacteria in Blood Culture-Like Conditions.Sci Rep. 2017 Aug 25;7(1):9457. doi: 10.1038/s41598-017-10072-z. Sci Rep. 2017. PMID: 28842712 Free PMC article.
-
Fever and infections in surgical intensive care: an American Association for the Surgery of Trauma Critical Care Committee clinical consensus document.Trauma Surg Acute Care Open. 2024 Jun 3;9(1):e001303. doi: 10.1136/tsaco-2023-001303. eCollection 2024. Trauma Surg Acute Care Open. 2024. PMID: 38835635 Free PMC article.
References
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2334/14/489/prepub
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
