

Impact of tumor location and pathological discordance on survival of children with midline high-grade gliomas treated on Children's Cancer Group high-grade glioma study CCG-945
- PMID: 25431150
- PMCID: PMC4323766
- DOI: 10.1007/s11060-014-1669-x
Impact of tumor location and pathological discordance on survival of children with midline high-grade gliomas treated on Children's Cancer Group high-grade glioma study CCG-945
Abstract
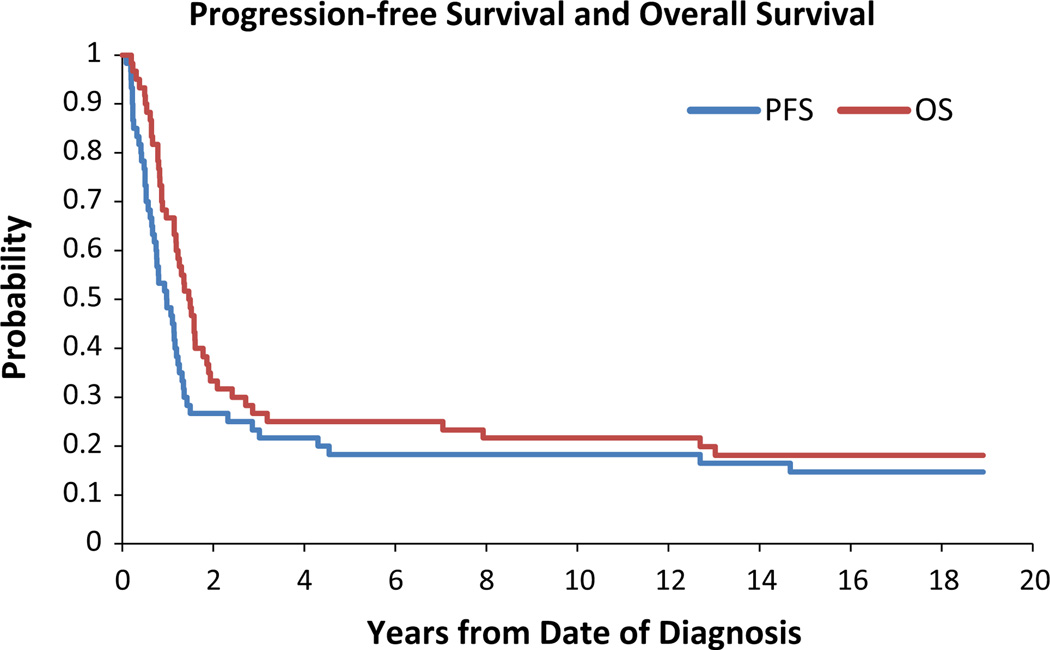
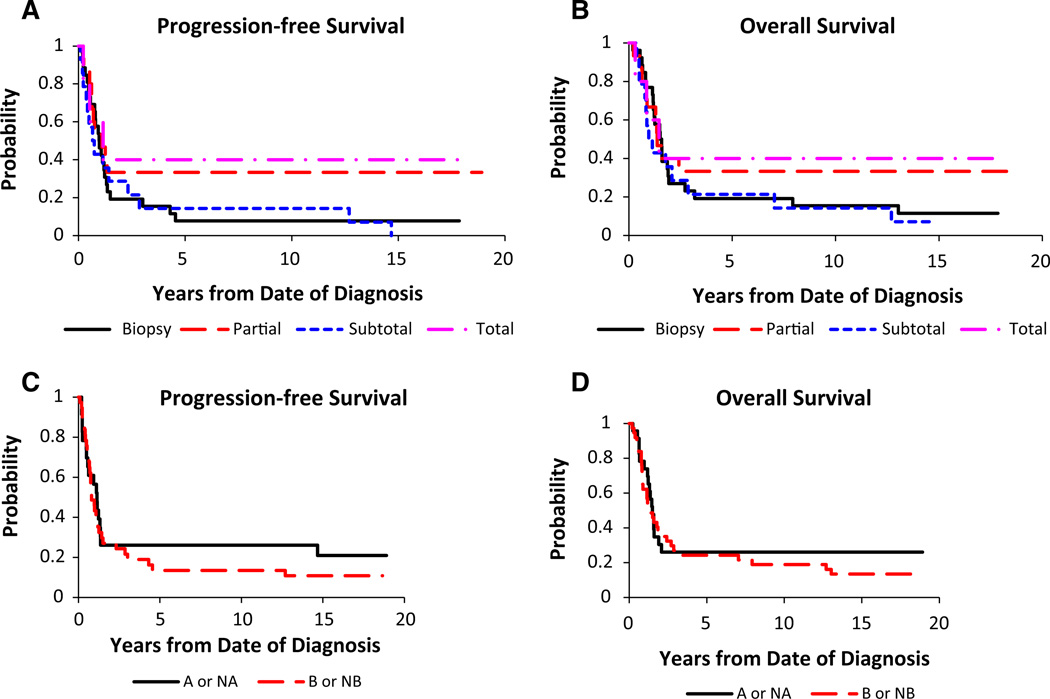
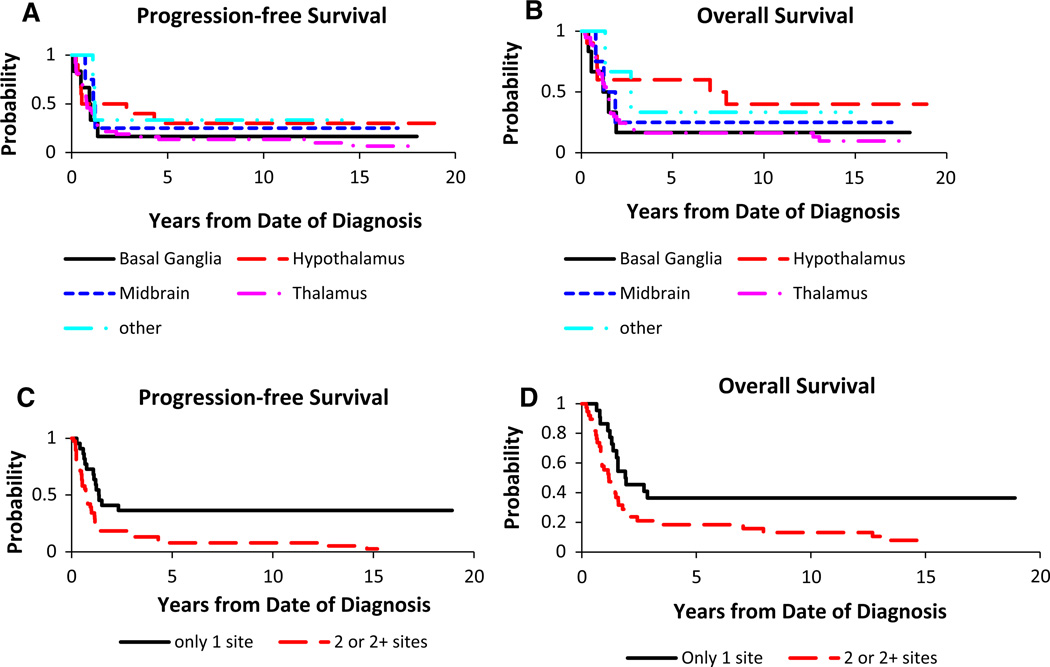
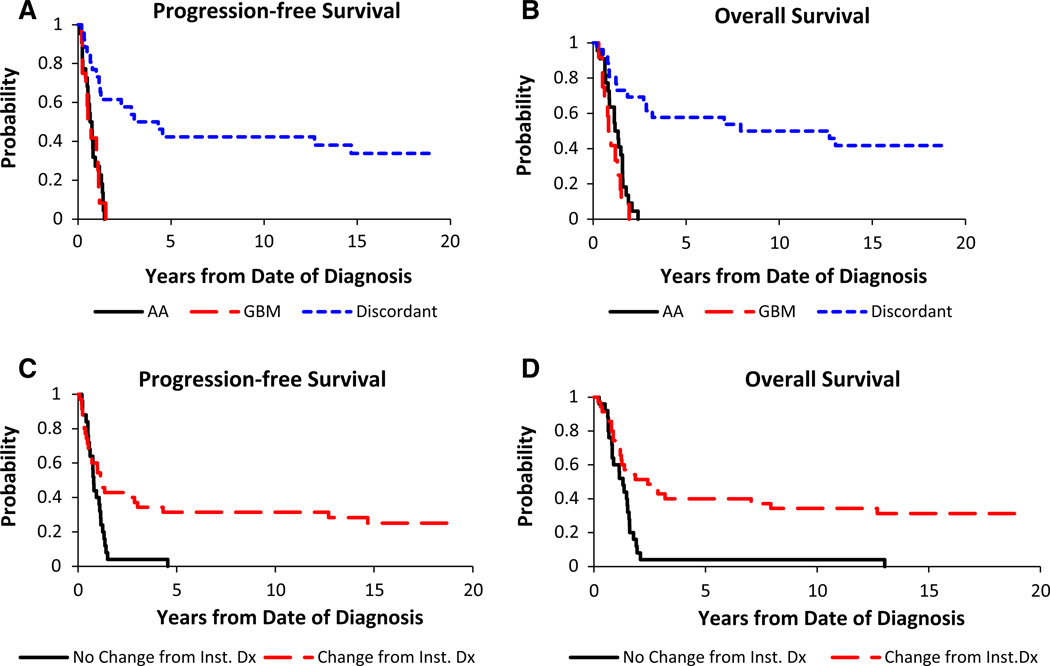
Children with high-grade glioma (HGG) have a poor prognosis compared to those with low-grade glioma (LGG). Adjuvant chemotherapy may be beneficial, but its optimal use remains undetermined. Histology and extent of resection are important prognostic factors. We tested the hypothesis that patients with midline HGG treated on Children's Cancer Group Study (CCG) CCG-945 have a worse prognosis compared to the entire group. Of 172 children eligible for analysis, 60 had midline tumors primarily localized to the thalamus, hypothalamus and basal ganglia. Time-to-progression and death were determined from the date of initial diagnosis, and survival curves were calculated. Univariate analyses were undertaken for extent of resection, chemotherapy regimen, anatomic location, histology, proliferation index, MGMT status and p53 over-expression. For the entire midline tumor group, 5-year PFS and OS were 18.3 ± 4.8 and 25 ± 5.4 %, respectively. Many patients only had a biopsy (43.3 %). The sub-groups with near/total resection and hypothalamic location appeared to have better PFS and OS. However, the effect of tumor histology on OS was significant for children with discordant diagnoses on central pathology review of LGG compared to HGG. Proliferative index (MIB-1 > 36 %), MGMT and p53 over-expression correlated with poor outcomes. Children treated on CCG-945 with midline HGG have a worse prognosis when compared to the entire group. The midline location may directly influence the extent of resection. Central pathology review and entry of patients on clinical trials continue to be priorities to improve outcomes for children with HGG.
Conflict of interest statement
Figures
References
-
- Sposto R, Ertel IJ, Jenkin RD, Boesel CP, Venes JL, Ortega JA, Evans AE, Wara W, Hammond D. The effectiveness of chemotherapy for treatment of high grade astrocytoma in children: results of a randomized trial. A report from the Children’s Cancer Study Group. J Neurooncol. 1989;7:165–177. - PubMed
-
- Finlay JL, Boyett JM, Yates AJ, Wisoff JH, Milstein JM, Geyer JR, Bertolone SJ, McGuire P, Cherlow JM, Tefft M, et al. Randomized phase III trial in childhood high-grade astrocytoma comparing vincristine, lomustine, and prednisone with the eight-drugs-in-1-day regimen. Children’s Cancer Group. J Clin Oncol. 1995;13:112–123. - PubMed
-
- Pollack IF, Hamilton RL, Burnham J, Holmes EJ, Finkelstein SD, Sposto R, Yates AJ, Boyett JM, Finlay JL. Impact of proliferation index on outcome in childhood malignant gliomas: results in a multi-institutional cohort. Neurosurgery. 2002;50:1238–1244. discussion 1244–1235. - PubMed
-
- Pollack IF, Hamilton RL, Sobol RW, Burnham J, Yates AJ, Holmes EJ, Zhou T, Finlay JL. O6-methylguanine-DNA methyltransferase expression strongly correlates with outcome in childhood malignant gliomas: results from the CCG-945 Cohort. J Clin Oncol. 2006;24:3431–3437. - PubMed
-
- Pollack IF, Finkelstein SD, Woods J, Burnham J, Holmes EJ, Hamilton RL, Yates AJ, Boyett JM, Finlay JL, Sposto R. Expression of p53 and prognosis in children with malignant gliomas. N Engl J Med. 2002;346:420–427. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
