

Increasing Obesity in Treated Female HIV Patients from Sub-Saharan Africa: Potential Causes and Possible Targets for Intervention
- PMID: 25431572
- PMCID: PMC4230180
- DOI: 10.3389/fimmu.2014.00507
Increasing Obesity in Treated Female HIV Patients from Sub-Saharan Africa: Potential Causes and Possible Targets for Intervention
Abstract
Objectives: To investigate changing nutritional demographics of treated HIV-1-infected patients and explore causes of obesity, particularly in women of African origin.
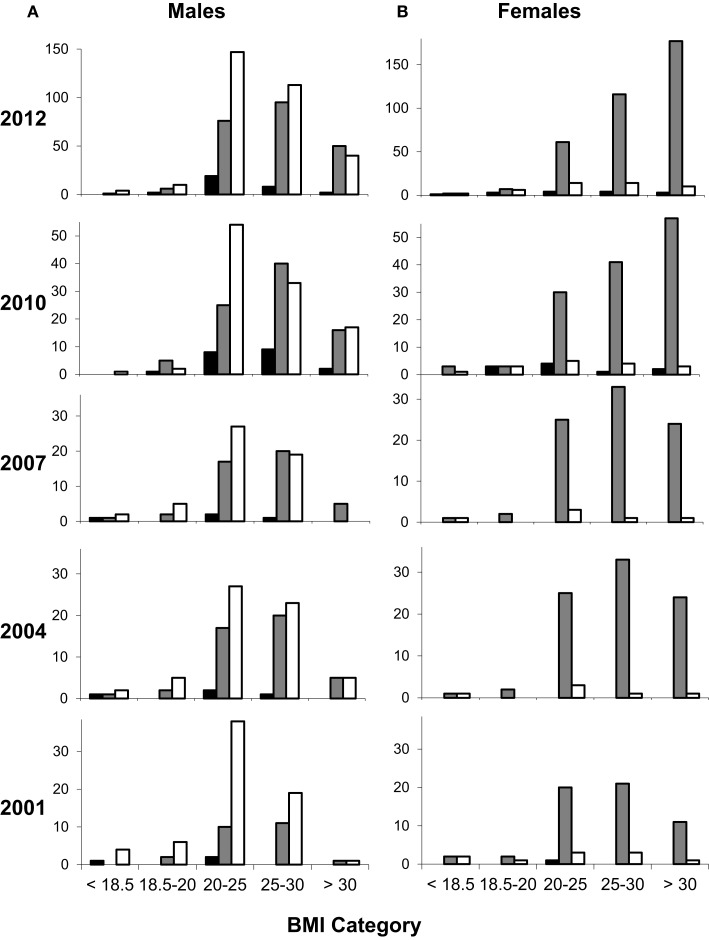
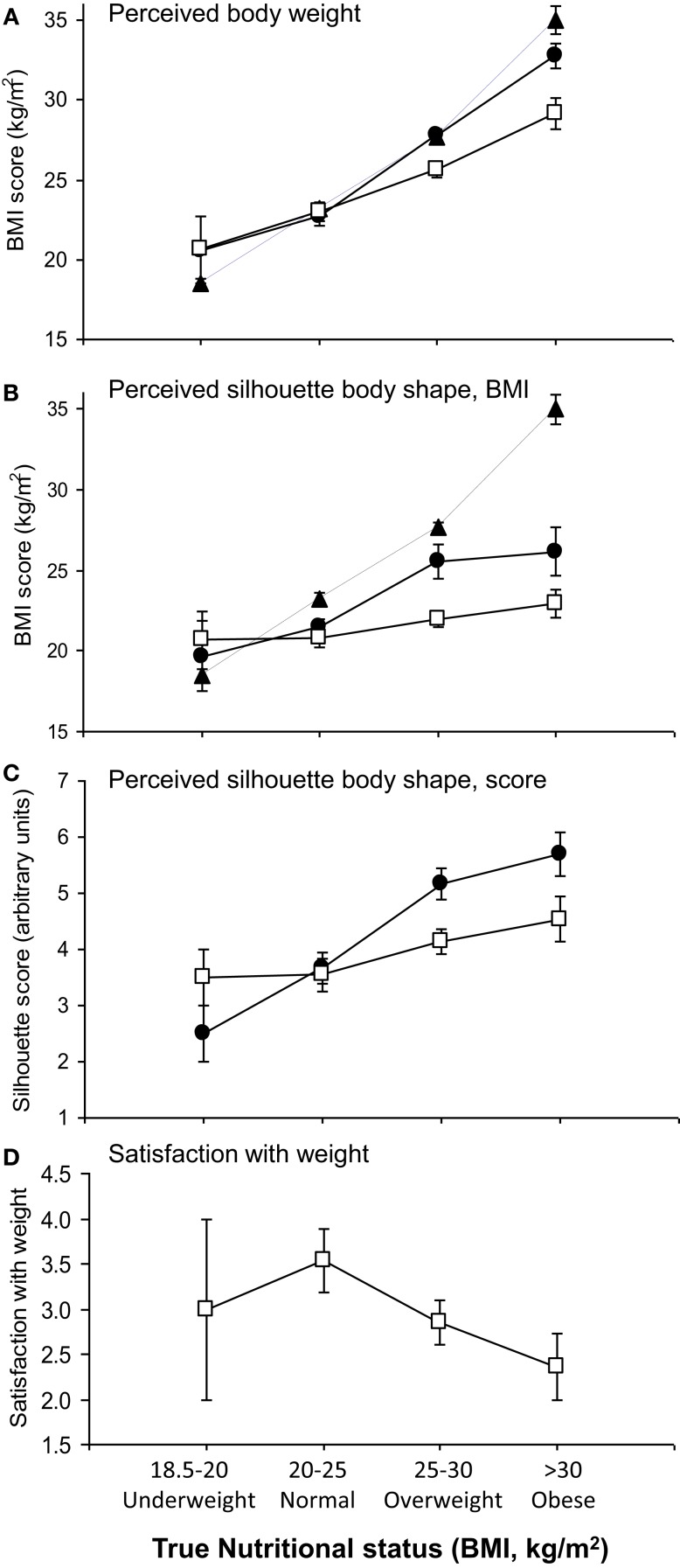
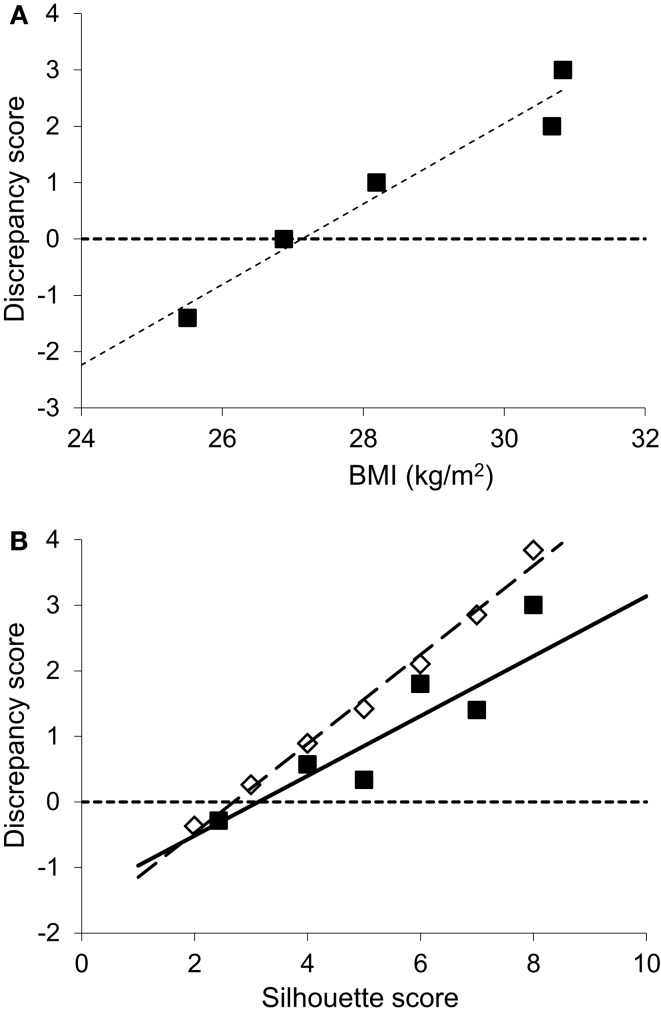
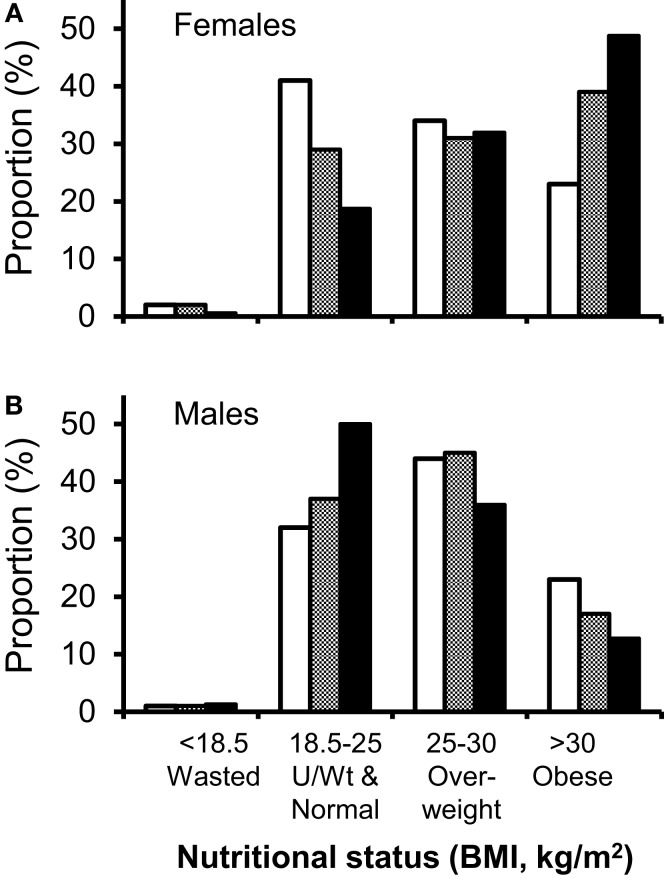
Methods: We prospectively reviewed nutritional demographics of clinic attenders at an urban European HIV clinic during four one-month periods at three-yearly intervals (2001, 2004, 2007, and 2010) and in two consecutive whole-year reviews (2010-2011 and 2011-2012). Risk-factors for obesity were assessed by multiple linear regression. A sub-study of 50 HIV-positive African female patients investigated body-size/shape perception using numerical, verbal, and pictorial cues.
Results: We found a dramatic rise in the prevalence of obesity (BMI > 30 kg/m(2)), from 8.5 (2001) to 28% (2011-2012) for all clinic attenders, of whom 86% were on antiretroviral treatment. Women of African origin were most affected, 49% being obese, with a further 32% overweight (BMI 25-30 kg/m(2)) in 2012. Clinical factors strongly associated with obesity included female gender, black African ethnicity, non-smoking, age, and CD4 count (all P < 0.001); greater duration of cART did not predict obesity. Individual weight-time trends mostly showed slow long-term progressive weight gain. Investigating body-weight perception, we found that weight and adiposity were underestimated by obese subjects, who showed a greater disparity between perceived and actual adiposity (P < 0.001). Obese subjects targeted more obese target "ideal" body shapes (P < 0.01), but were less satisfied with their body shape overall (P = 0.02).
Conclusion: Seropositive African women on antiretroviral treatment are at heightened risk of obesity. Although multifactorial, body-weight perception represents a potential target for intervention.
Keywords: HIV; HIV-associated lipodystrophy syndrome; antiretroviral treatment; body mass index; body weight; ethnology; obesity.
Figures
References
-
- Sabin CA, Worm SW, Weber R, Reiss P, El-Sadr W, Dabis F, et al. Use of nucleoside reverse transcriptase inhibitors and risk of myocardial infarction in HIV-infected patients enrolled in the D:A:D study: a multi-cohort collaboration. Lancet (2008) 371(9622):1417–26.10.1016/S0140-6736(08)60423-7 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials