

Antibiotics in fetal and early life and subsequent childhood asthma: nationwide population based study with sibling analysis
- PMID: 25432937
- PMCID: PMC4247260
- DOI: 10.1136/bmj.g6979
Antibiotics in fetal and early life and subsequent childhood asthma: nationwide population based study with sibling analysis
Erratum in
- BMJ. 2014;349:g7395
Abstract
Objective: To investigate the association between exposure to antibiotics in fetal and early life and asthma in childhood, with adjustment for confounding factors.
Design: Nationwide prospective population based cohort study, including sibling control design.
Setting: Swedish population identified from national demographic and health registers.
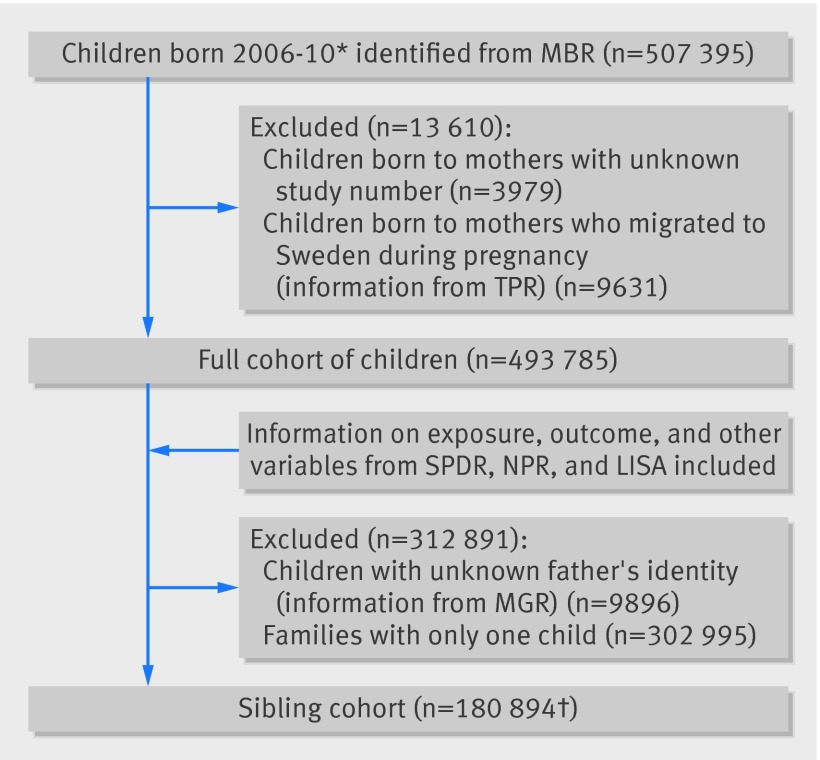
Participants: 493,785 children born 2006-10; 180,894 of these were eligible for sibling analyses.
Main outcome measure: Asthma defined as having both an asthma diagnosis and dispensed asthma drugs. The association between antibiotic exposure and asthma was investigated in the whole cohort with Cox proportional hazard regression. A stratified proportional hazards model conditional on sibling group was used to adjust for shared factors within families. Confounding by respiratory infections was assessed by investigating whether specific groups of antibiotics were associated with asthma.
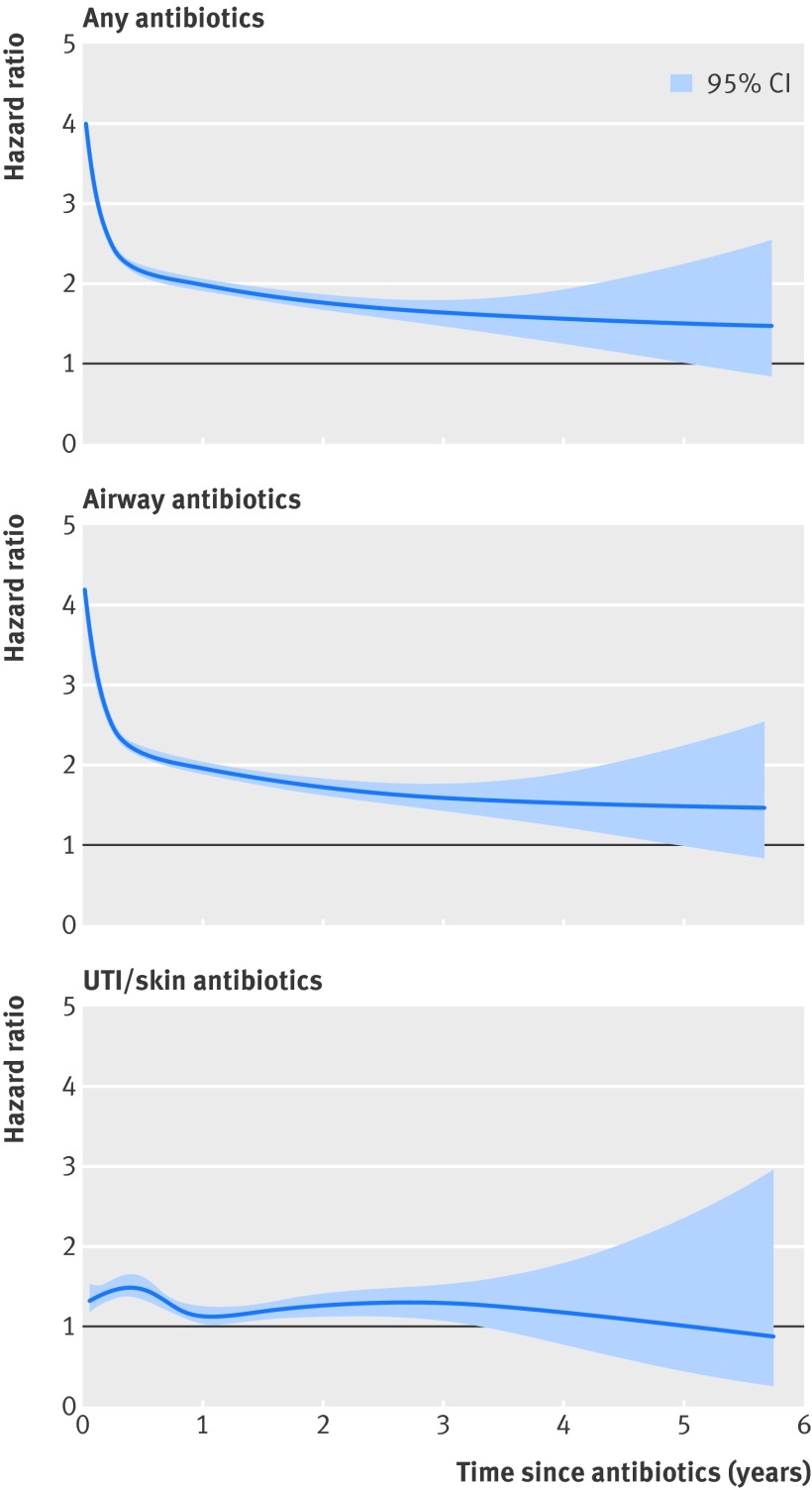
Results: Antibiotic exposure in fetal life was associated with an increased risk of asthma in cohort analyses (hazard ratio 1.28, 95% confidence interval 1.25 to 1.32), but not in sibling analyses (0.99, 0.92 to 1.07). In cohort analyses, antibiotics used to treat respiratory infections in childhood were associated with a more pronounced increased risk of asthma (4.12, 3.78 to 4.50) than antibiotics used for urinary tract and skin infections (1.54, 1.24 to 1.92). In sibling analyses, the excess risks after exposure to antibiotics for respiratory infections decreased (2.36, 1.78 to 3.13) and disappeared for antibiotics for urinary tract and skin (0.85, 0.47 to 1.55).
Conclusions: Previous positive associations between exposure to antibiotics in fetal and early life and subsequent childhood asthma could have been caused by confounding by shared familial factors, in addition to confounding by respiratory infections.
© Örtqvist et al 2014.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Adriaenssens N, Coenen S, Versporten A, Muller A, Minalu G, Faes C, et al. European Surveillance of Antimicrobial Consumption (ESAC): outpatient antibiotic use in Europe (1997-2009). J Antimicrob Chemother 2011;66:3-12. - PubMed
-
- Asher MI, Montefort S, Bjorksten B, Lai CK, Strachan DP, Weiland SK, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet 2006;368:733-43. - PubMed
-
- McKeever TM, Lewis SA, Smith C, Hubbard R. The importance of prenatal exposures on the development of allergic disease: a birth cohort study using the West Midlands General Practice Database. Am J Respir Crit Care Med 2002;166:827-32. - PubMed
-
- Rusconi F, Galassi C, Forastiere F, Bellasio M, De Sario M, Ciccone G, et al. Maternal complications and procedures in pregnancy and at birth and wheezing phenotypes in children. Am J Respir Crit Care Med 2007;175:16-21. - PubMed
-
- Stensballe LG, Simonsen J, Jensen SM, Bonnelykke K, Bisgaard H. Use of antibiotics during pregnancy increases the risk of asthma in early childhood. J Pediatr 2013;162:832-8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical