

Survival analysis of pelvic lymphadenectomy alone versus combined pelvic and para-aortic lymphadenectomy in patients exhibiting endometrioid type endometrial cancer
- PMID: 25435992
- PMCID: PMC4246997
- DOI: 10.3892/ol.2014.2653
Survival analysis of pelvic lymphadenectomy alone versus combined pelvic and para-aortic lymphadenectomy in patients exhibiting endometrioid type endometrial cancer
Abstract
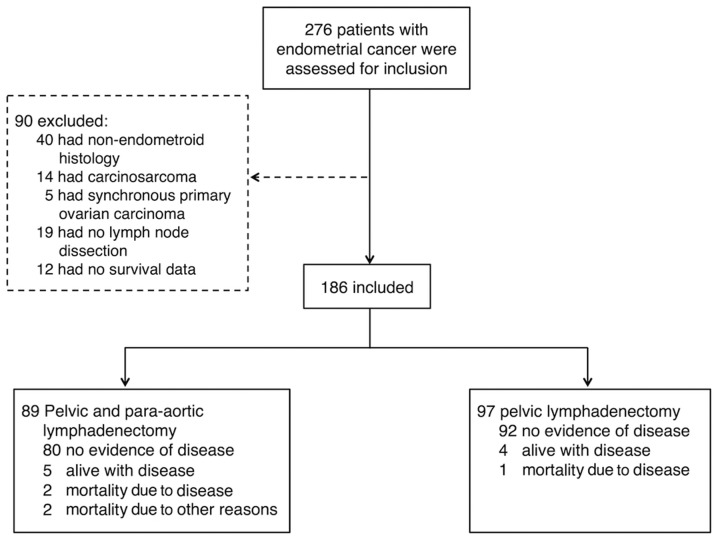
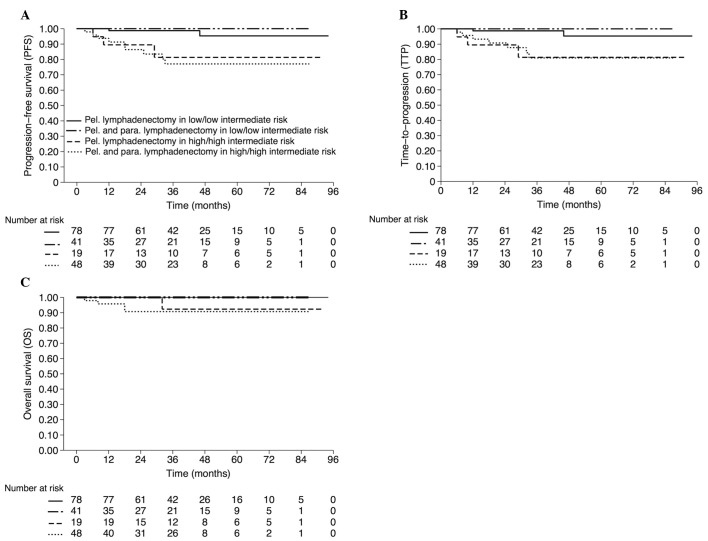
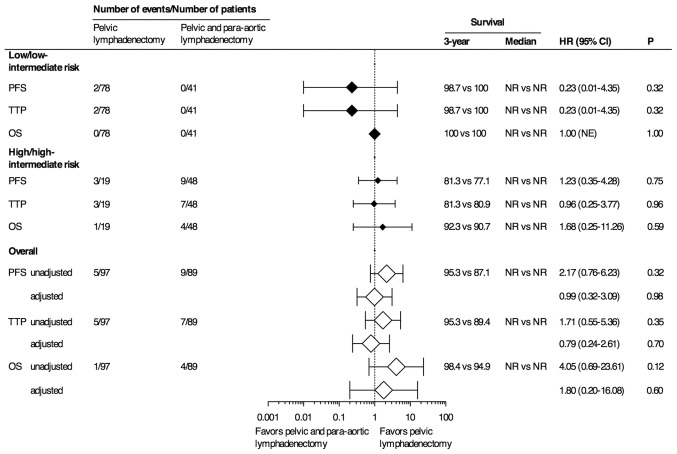
The therapeutic benefit of lymphadenectomy in patients exhibiting endometrial cancer (EC) remains controversial. The aim of the present study was to determine whether the addition of para-aortic lymphadenectomy to pelvic lymphadenectomy (PLND) improves survival in patients with endometrioid type EC. A single tertiary-center, retrospective analysis was conducted in a total of 186 patients who were surgically treated with either PLND alone (n=97) or combined pelvic and para-aortic lymphadenectomy (PPaLND; n=89). Adjuvant treatments were assigned according to the Gynecologic Oncology Group (GOG) risk of recurrence analysis. The primary endpoint of the present study was progression-free survival (PFS). The median follow-up time was 38 months (95% confidence interval, 36.47-42.90) for all patients. No statistically significant differences were identified between the two groups in terms of overall survival (OS), PFS or time to progression (TTP). Kaplan-Meier estimates of three-year OS, PFS and TTP for patients with low or low-intermediate risk were as follows: PLND, 100, 98.7 and 98.7%, respectively; and PPaLND, all 100%. The estimated three-year OS, PFS and TTP for patients with high or high-intermediate risk were as follows: PLND, 92.3, 81.3 and 81.3%; and PPaLND, 90.7, 77.1 and 80.9%, respectively. No statistically significant differences were detected in the three-year OS, PFS and TTP between the lymphadenectomy groups, regardless of the GOG risk of recurrence (PLND, 98.4, 95.3 and 95.3%; and PPaLND, 94.9, 87.1 and 89.4%). Therefore, the combination treatment, PPaLND did not provide any survival advantage over pelvic lymphadenectomy alone.
Keywords: endometrial cancer; endometrioid type; lymphadenectomy; survival.
Figures
References
-
- FIGO. Classification and staging of malignant tumours in the female pelvis. Int J Gynaecol Obstet. 1989;28:190. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases