

Consensus review of the treatment of cardiovascular disease in people with hemophilia A and B
- PMID: 25436468
- PMCID: PMC4323575
- DOI: 10.1097/CRD.0000000000000045
Consensus review of the treatment of cardiovascular disease in people with hemophilia A and B
Abstract
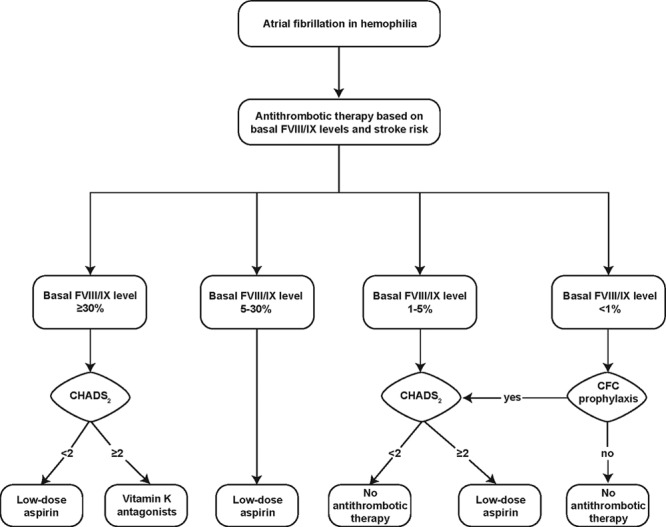
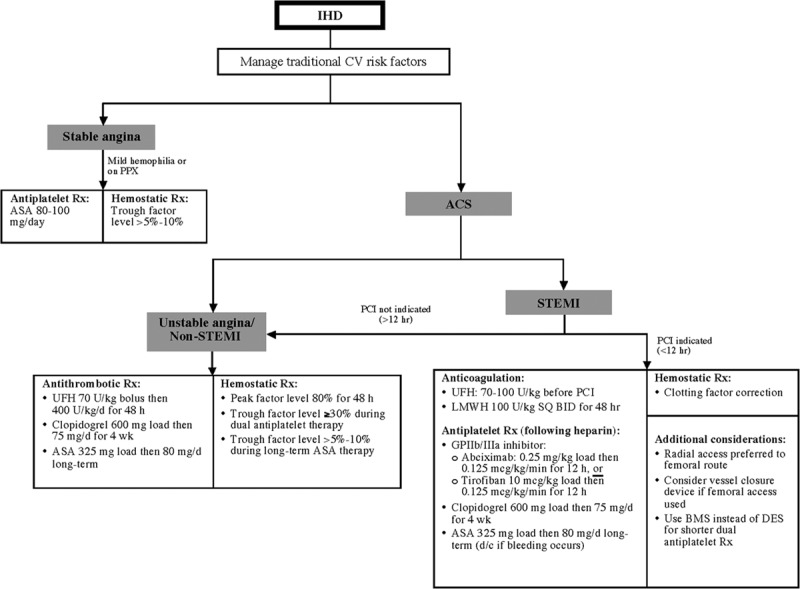
With advances in care, increasing numbers of people with hemophilia (PWH) achieve near-normal life expectancies and present with typical age-related cardiovascular conditions. Evidence-based guidelines for medical or surgical management of cardiovascular conditions in individuals with hemophilia are limited. Published recommendations exist for the management of some common cardiovascular conditions (eg, ischemic heart disease, atrial fibrillation), but identifying optimal strategies for anticoagulant or antithrombotic therapy constitutes the primary challenge of managing nonoperative cardiovascular disease (CVD) in PWH. In general, as long as factor concentrates or other hemostatic therapies maintain adequate hemostasis, the recommended medical and surgical management of CVD in PWH parallels that in individuals without hemophilia. The presence of factor inhibitors complicates hemophilia management. Published outcomes of CVD treatment in PWH are similar to those in the general population. Specific knowledge about factor replacement, factor inhibitors, and disease-specific treatment distinguishes the cardiovascular care of PWH from similar care of individuals without this rare bleeding disorder. Furthermore, a multidisciplinary approach incorporating a hematologist with an onsite coagulation laboratory, ideally associated with a hemophilia treatment center, is integral to the management of CVD in PWH.
Conflict of interest statement
Disclosure: Victor A. Ferraris has been a paid consultant for Baxter Healthcare (CME activity), Haemonetics (advisory board), and AstraZeneca (advisory board). Leonard I. Boral has previously been a paid consultant for Alexion Pharmaceuticals. Alice J. Cohen and Susan S. Smyth declare no competing interests. Gilbert C. White is a paid consultant for Bayer (grant review); Baxter (Data Safety Monitoring Board); and CSL Behring, Novo Nordisk, and Pfizer (advisory boards); is a cofounder of and scientific advisory board member for Entegrion; and is on the scientific advisory board for Asklepios.
Figures
References
-
- Boggio LN, Kessler CM. Hemophilia A and B. In: Kitchens CS, Alving BM, Kessler CM, editors. In: Consultative Hemostasis and Thrombosis. 2nd ed. Philadelphia: Elsevier Health Sciences; 2007. pp. 45–59.
-
- Kulkarni R, Soucie JM. Pediatric hemophilia: a review. Semin Thromb Hemost. 2011;37:737–744. - PubMed
-
- DiMichele DM. Inhibitors in Hemophilia: A Primer. 4th ed. Montreal: World Federation of Hemophilia; 2008.
-
- Bolton-Maggs PH, Pasi KJ. Haemophilias A and B. Lancet. 2003;361:1801–1809. - PubMed
-
- Goedert JJ, Eyster ME, Lederman MM, et al. End-stage liver disease in persons with hemophilia and transfusion-associated infections. Blood. 2002;100:1584–1589. - PubMed
