

Randomized placebo-controlled phase II trial of autologous mesenchymal stem cells in multiple sclerosis
- PMID: 25436769
- PMCID: PMC4250058
- DOI: 10.1371/journal.pone.0113936
Randomized placebo-controlled phase II trial of autologous mesenchymal stem cells in multiple sclerosis
Abstract
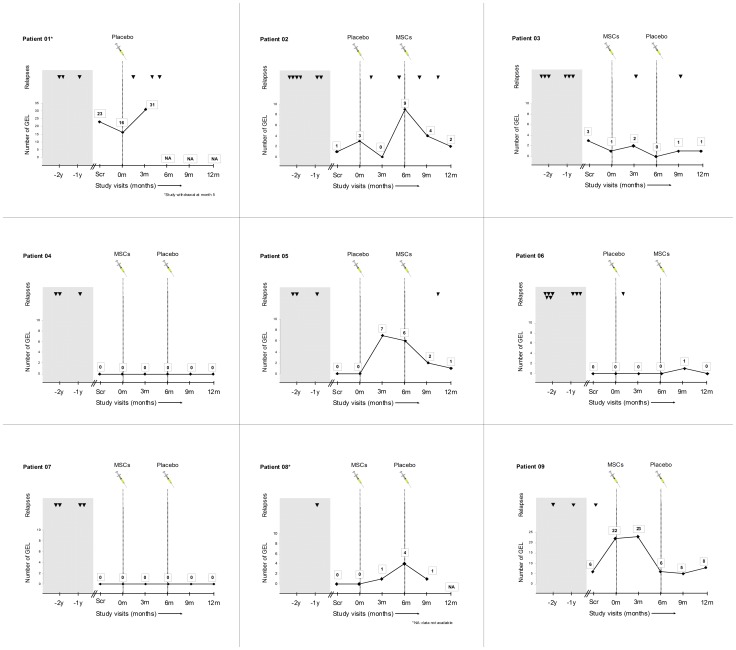
Objective: Uncontrolled studies of mesenchymal stem cells (MSCs) in multiple sclerosis suggested some beneficial effect. In this randomized, double-blind, placebo-controlled, crossover phase II study we investigated their safety and efficacy in relapsing-remitting multiple sclerosis patients. Efficacy was evaluated in terms of cumulative number of gadolinium-enhancing lesions (GEL) on magnetic resonance imaging (MRI) at 6 months and at the end of the study.
Methods: Patients unresponsive to conventional therapy, defined by at least 1 relapse and/or GEL on MRI scan in past 12 months, disease duration 2 to 10 years and Expanded Disability Status Scale (EDSS) 3.0-6.5 were randomized to receive IV 1-2×10(6) bone-marrow-derived-MSCs/Kg or placebo. After 6 months, the treatment was reversed and patients were followed-up for another 6 months. Secondary endpoints were clinical outcomes (relapses and disability by EDSS and MS Functional Composite), and several brain MRI and optical coherence tomography measures. Immunological tests were explored to assess the immunomodulatory effects.
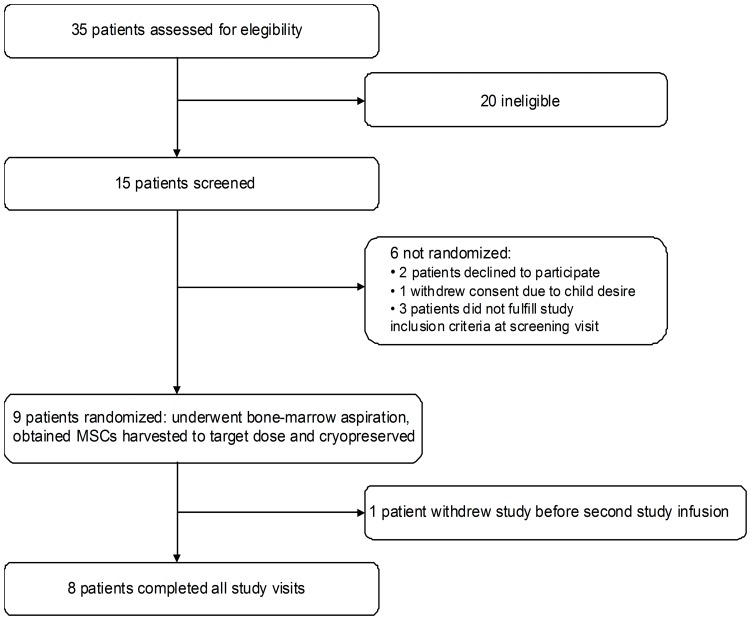
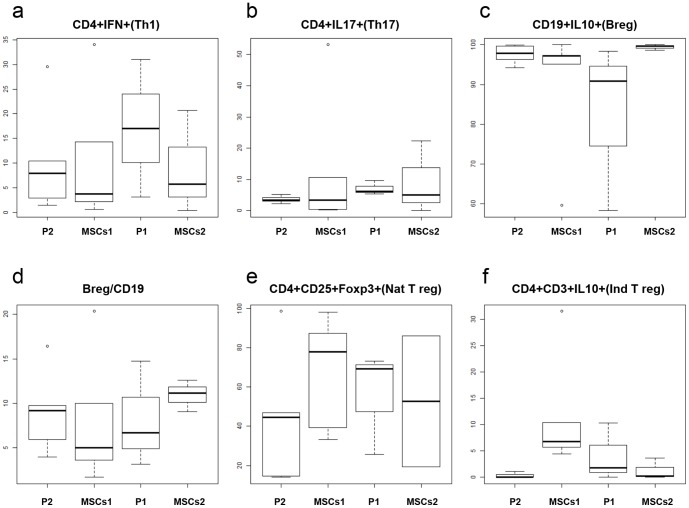
Results: At baseline 9 patients were randomized to receive MSCs (n = 5) or placebo (n = 4). One patient on placebo withdrew after having 3 relapses in the first 5 months. We did not identify any serious adverse events. At 6 months, patients treated with MSCs had a trend to lower mean cumulative number of GEL (3.1, 95% CI = 1.1-8.8 vs 12.3, 95% CI = 4.4-34.5, p = 0.064), and at the end of study to reduced mean GEL (-2.8±5.9 vs 3±5.4, p = 0.075). No significant treatment differences were detected in the secondary endpoints. We observed a non-significant decrease of the frequency of Th1 (CD4+ IFN-γ+) cells in blood of MSCs treated patients.
Conclusion: Bone-marrow-MSCs are safe and may reduce inflammatory MRI parameters supporting their immunomodulatory properties. ClinicalTrials.gov NCT01228266.
Conflict of interest statement
Figures
References
-
- Uccelli A, Laroni A, Freedman MS (2011) Mesenchymal stem cells for the treatment of multiple sclerosis and other neurological diseases. Lancet Neurol 10:649–656. - PubMed
-
- Rice CM, Kemp K, Wilkins A, Scolding NJ (2013) Cell therapy for multiple sclerosis: an evolving concept with implications for other neurodegenerative diseases. Lancet 382:1204–1213. - PubMed
-
- Yamout B, Hourani R, Salti H, Barada W, El-Hajj T, et al. (2010) Bone marrow mesenchymal stem cell transplantation in patients with multiple sclerosis: a pilot study. J Neuroimmunol 227:185–189. - PubMed
-
- Rice CM, Mallam EA, Whone AL, Walsh P, Brooks DJ, et al. (2010) Safety and feasibility of autologous bone marrow cellular therapy in relapsing-progressive multiple sclerosis. Clin Pharmacol Ther 87:679–685. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
