

Is the learning curve of robotic low anterior resection shorter than laparoscopic low anterior resection for rectal cancer?: a comparative analysis of clinicopathologic outcomes between robotic and laparoscopic surgeries
- PMID: 25437022
- PMCID: PMC4616378
- DOI: 10.1097/MD.0000000000000109
Is the learning curve of robotic low anterior resection shorter than laparoscopic low anterior resection for rectal cancer?: a comparative analysis of clinicopathologic outcomes between robotic and laparoscopic surgeries
Abstract
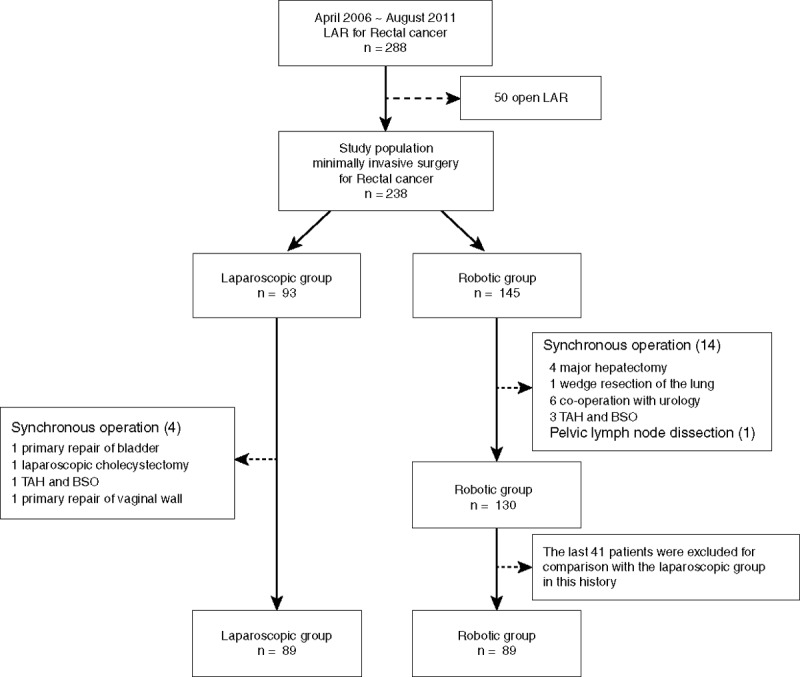
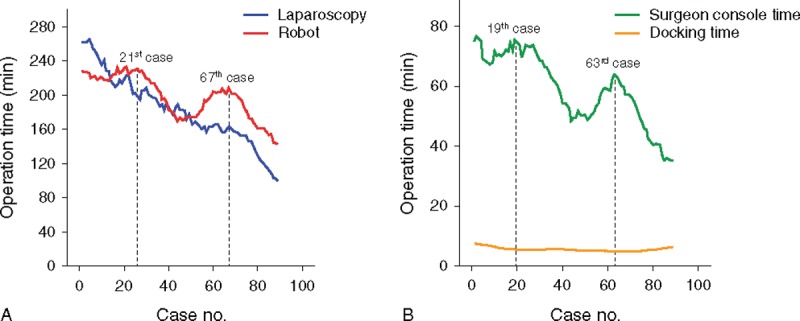
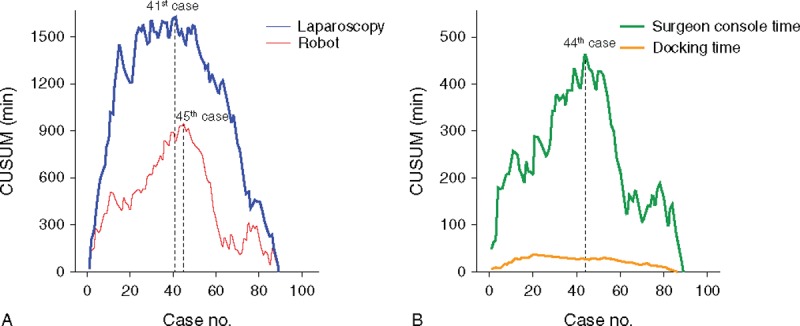
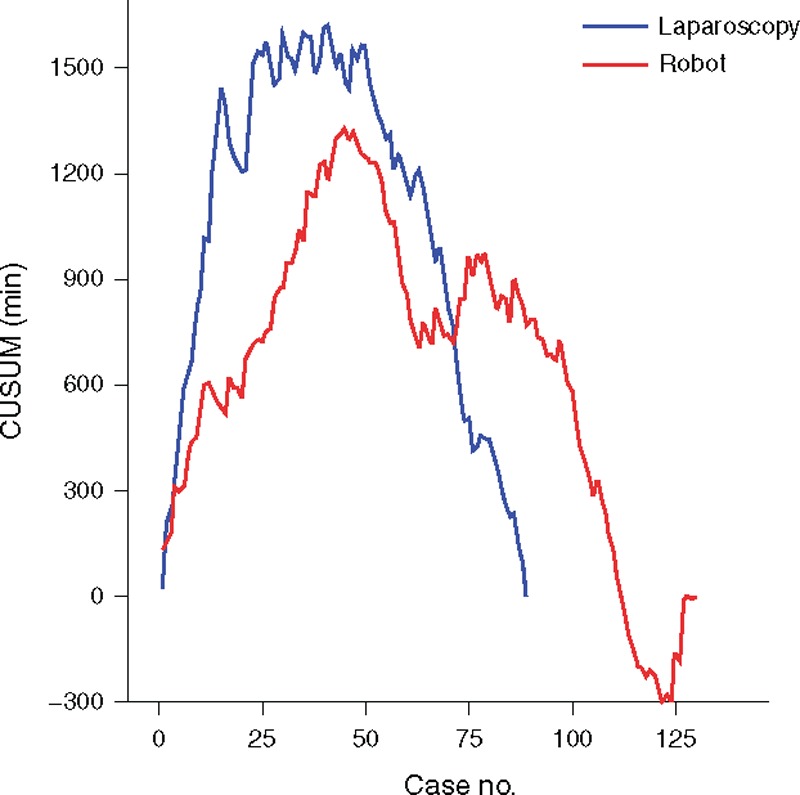
As robotic surgery was developed with ergonomic designs, there are expectations that the technical advantages of robotic surgery can shorten the learning curve. However, there is no comparative study, so far, to evaluate the learning curve between robotic and laparoscopic rectal cancer surgeries. Therefore, the aim of this study is to compare the learning curve of robotic low anterior resection (LAR) with laparoscopic LAR for rectal cancer.Patients who underwent robotic or laparoscopic LAR by a single surgeon were compared retrospectively (robot n = 89 vs laparoscopy n = 89). Cumulative sum (CUSUM) was used to evaluate the learning curve. The patients were divided into phase 1 (initial learning curve period) and phase 2 (post-learning curve period). The perioperative clinicopathologic characteristics were compared by phases and surgical procedures.According to CUSUM, the learning curve of robotic LAR was the 44th case and laparoscopic LAR was the 41st case. The learning phases were divided as follows: phase 1 (cases 1-41) versus phase 2 (cases 42-89) in the laparoscopic group, and phase 1 (cases 1-44) versus phase 2 (cases 45-89) in the robotic group. Comparison between phase 1 and phase 2 in each type of surgery showed no significant difference for the perioperative outcomes. Comparison between robotic and laparoscopic surgeries in each phase showed similar perioperative results. Pathologic outcomes were not significantly different in both procedures and phases.The learning curve of robotic LAR for rectal cancer was similar to laparoscopic LAR, and the clinicopathologic outcomes were similar in both the procedures.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Ng SS, Lee JF, Yiu RY, et al. Long-term oncologic outcomes of laparoscopic versus open surgery for rectal cancer: a pooled analysis of 3 randomized controlled trials. Ann Surg. 2014;259:139–147. - PubMed
-
- Jayne DG, Thorpe HC, Copeland J, et al. Five-year follow-up of the Medical Research Council CLASICC trial of laparoscopically assisted versus open surgery for colorectal cancer. Br J Surg. 2010;97:1638–1645. - PubMed
-
- Green BL, Marshall HC, Collinson F, et al. Long-term follow-up of the Medical Research Council CLASICC trial of conventional versus laparoscopically assisted resection in colorectal cancer. Br J Surg. 2013;100:75–82. - PubMed
-
- Group TCOoSTS. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med. 2004;350:2050–2059. - PubMed
-
- Miskovic D, Ni M, Wyles SM, et al. Learning curve and case selection in laparoscopic colorectal surgery: systematic review and international multicenter analysis of 4852 cases. Dis Colon Rectum. 2012;55:1300–1310. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
