

Development of a prediction rule for estimating postoperative pulmonary complications
- PMID: 25437175
- PMCID: PMC4249954
- DOI: 10.1371/journal.pone.0113656
Development of a prediction rule for estimating postoperative pulmonary complications
Abstract
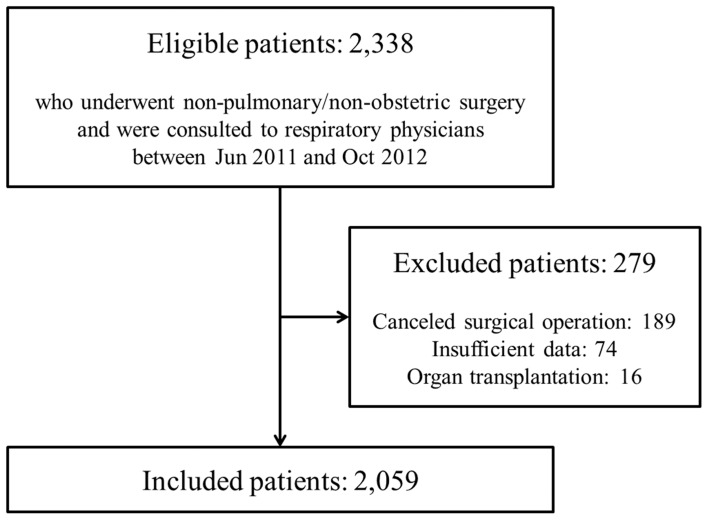
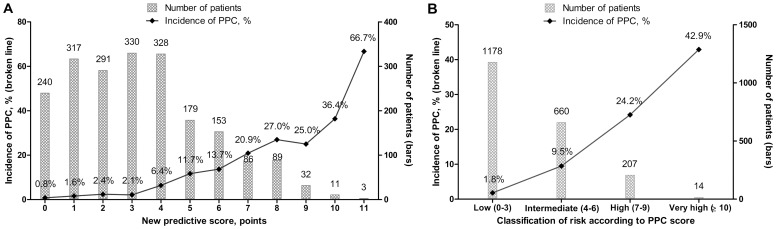
Patient- and procedure-related factors associated with postoperative pulmonary complications (PPCs) have changed over the last decade. Therefore, we sought to identify independent risk factors of PPCs and to develop a clinically applicable scoring system. We retrospectively analyzed clinical data from 2,059 patients who received preoperative evaluations from respiratory physicians between June 2011 and October 2012. A new scoring system for estimating PPCs was developed using beta coefficients of the final multiple regression models. Of the 2,059 patients studied, 140 (6.8%) had PPCs. A multiple logistic regression model revealed seven independent risk factors (with scores in parentheses): age ≥70 years (2 points), current smoker (1 point), the presence of airflow limitation (1 point), American Society of Anesthesiologists class ≥2 (1 point), serum albumin <4 g/dL (1 point), emergency surgery (2 points), and non-laparoscopic abdominal/cardiac/aortic aneurysm repair surgery (4 points). The area under the curve was 0.79 (95% CI, 0.75-0.83) with the newly developed model. The new risk stratification including laparoscopic surgery has a good discriminative ability for estimating PPCs in our study cohort. Further research is needed to validate this new prediction rule.
Conflict of interest statement
Figures
References
-
- Smetana GW (1999) Preoperative pulmonary evaluation. N Engl J Med 340:937–944. - PubMed
-
- Fleischmann KE, Goldman L, Young B, Lee TH (2003) Association between cardiac and noncardiac complications in patients undergoing noncardiac surgery: outcomes and effects on length of stay. Am J Med 115:515–520. - PubMed
-
- Fisher BW, Majumdar SR, McAlister FA (2002) Predicting pulmonary complications after nonthoracic surgery: a systematic review of blinded studies. Am J Med 112:219–225. - PubMed
-
- Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, et al. (1999) Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 100:1043–1049. - PubMed
-
- Smetana GW, Lawrence VA, Cornell JE. American College of P (2006) Preoperative pulmonary risk stratification for noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 144:581–595. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
