

Efficacy of QuadroPulse rTMS for improving motor function after spinal cord injury: Three case studies
- PMID: 25437531
- PMCID: PMC4725792
- DOI: 10.1179/2045772314Y.0000000279
Efficacy of QuadroPulse rTMS for improving motor function after spinal cord injury: Three case studies
Abstract
Context/objective: To examine the effects of repetitive QuadroPulse transcranial magnetic stimulation (rTMS(QP)) on hand/leg function after spinal cord injury (SCI).
Design: Interventional proof-of-concept study.
Setting: University laboratory.
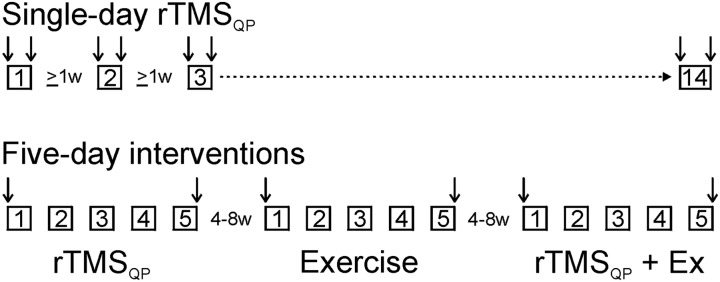
Participants: Three adult subjects with cervical SCI. Interventions Repeated trains of magnetic stimuli were applied to the motor cortical hand/leg area. Several exploratory single-day rTMS(QP) protocols were examined. Ultimately we settled on a protocol using three 5-day trials of (1) rTMS(QP) only; (2) exercise only (targeting hand or leg function); and (3) rTMS(QP) combined with exercise.
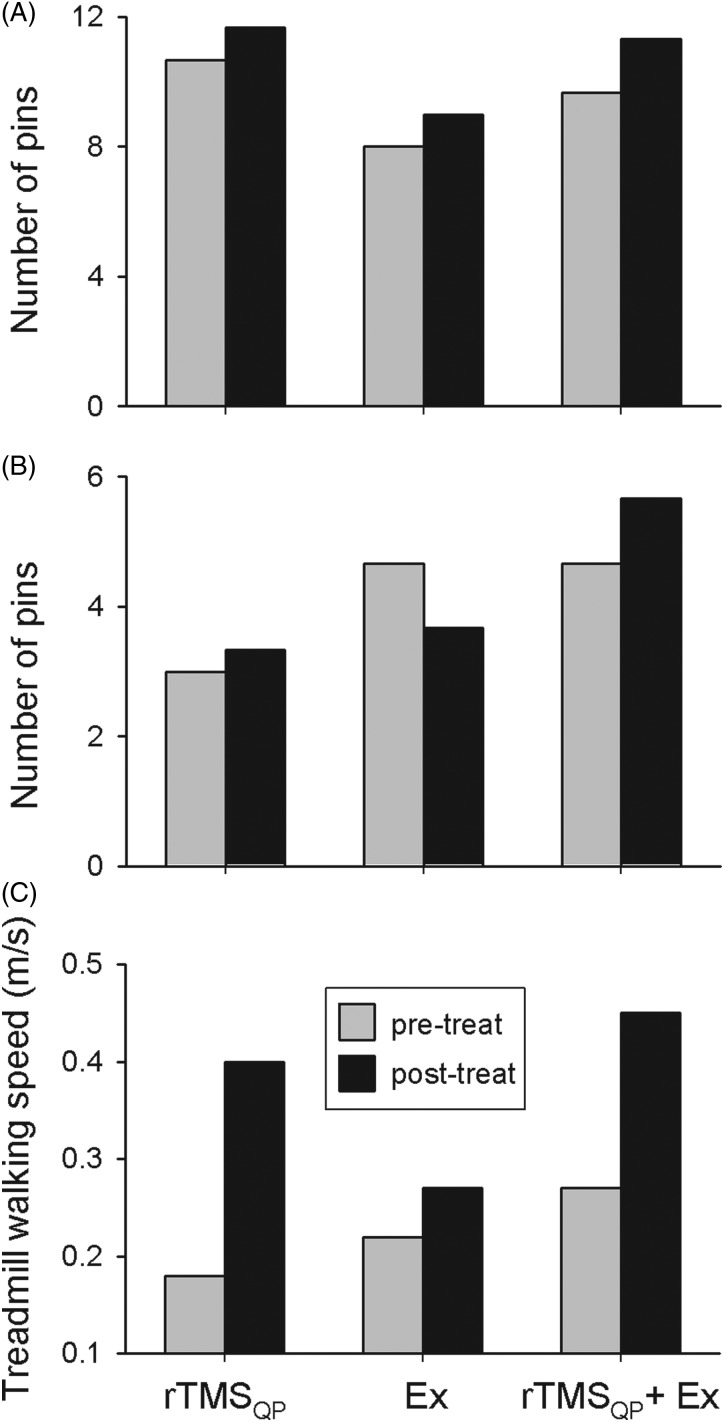
Outcome measures: Hand motor function was assessed by Purdue Pegboard and Complete Minnesota Dexterity tests. Walking function was based on treadmill walking and the Timed Up and Go test. Electromyographic recordings were used for neurophysiological testing of cortical (by single- and double-pulse TMS) and spinal (via tendon taps and electrical nerve stimulation) excitability.
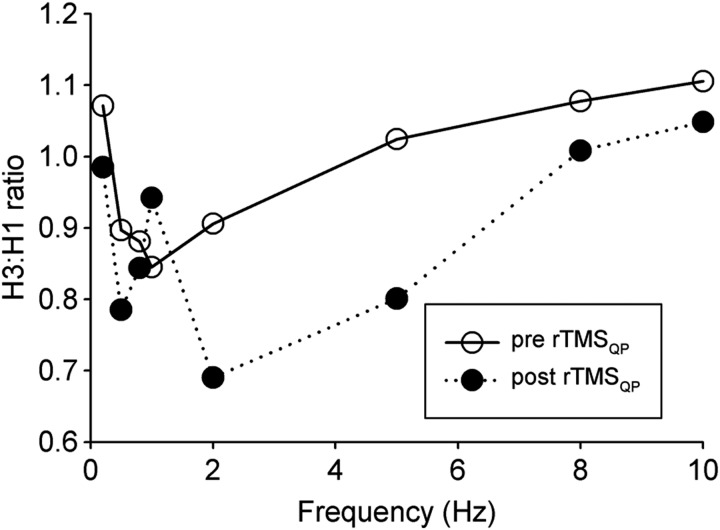
Results: Single-day rTMS(QP) application had no clear effect in the 2 subjects whose hand function was targeted, but improved walking speed in the person targeted for walking, accompanied by increased cortical excitability and reduced spinal excitability. All 3 subjects showed functional improvement following the 5-day rTMS(QP) intervention, an effect being even more pronounced after the five-day combined rTMS(QP) + exercise sessions. There were no rTMS(QP)-associated adverse effects.
Conclusion: Our findings suggest a functional benefit of motor cortical rTMS(QP) after SCI. The effect of rTMS(QP) appears to be augmented when stimulation is accompanied by targeted exercises, warranting expansion of this pilot study to a larger subject population.
Keywords: Motor function; Rehabilitation; Repetitive transcranial magnetic stimulation; Spinal cord injury.
Figures
References
-
- Nathan PW. Effects on movement of surgical incisions into the human spinal cord. Brain 1994;117(Pt 2):337–46. - PubMed
-
- Lemon RN. Descending pathways in motor control. Annu Rev Neurosci 2008;31:195–218. - PubMed
-
- Calancie B, Alexeeva N, Broton JG, Molano MR. Interlimb reflex activity after spinal cord injury in man: strengthening response patterns are consistent with ongoing synaptic plasticity. Clin Neurophysiol 2005;116(1):75–86. - PubMed
-
- Wrigley PJ, Gustin SM, Macey PM, Nash PG, Gandevia SC, Macefield VG, et al. Anatomical changes in human motor cortex and motor pathways following complete thoracic spinal cord injury. Cereb Cortex 2009;19(1):224–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical