

Benefits of dynamic susceptibility-weighted contrast-enhanced perfusion MRI for glioma diagnosis and therapy
- PMID: 25438812
- PMCID: PMC4277861
- DOI: 10.2217/cns.14.44
Benefits of dynamic susceptibility-weighted contrast-enhanced perfusion MRI for glioma diagnosis and therapy
Abstract
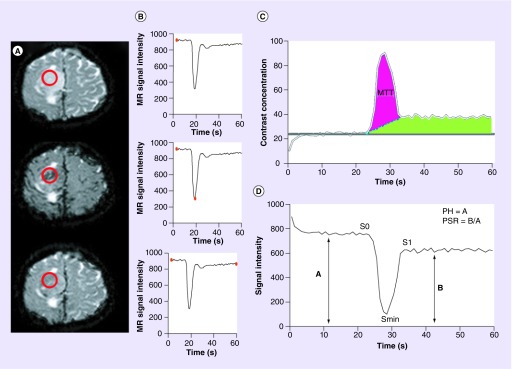
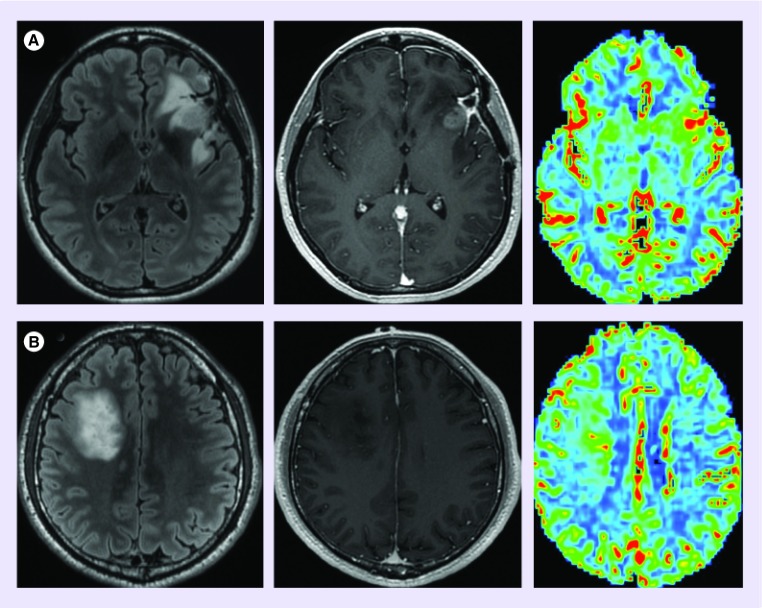
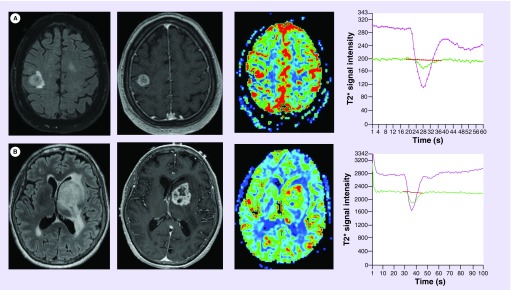
Glioma are the most common supra-tentorial brain tumor in the USA with an estimated annual incidence of 17,000 new cases per year. Dynamic susceptibility-weighted contrast-enhanced (DSC) perfusion MRI noninvasively characterizes tumor biology allowing for the diagnosis and therapeutic monitoring of glioma. This MRI technique utilizes the rapid changes in signal intensity caused by a rapid intravascular bolus of paramagnetic contrast agent to calculate physiologic perfusion metrics. DSC perfusion MRI has increasingly become an integrated part of glioma imaging. The specific aim of this article is to review the benefits of DSC perfusion MRI in the therapy of glioma.
Keywords: cerebral blood volume; dynamic susceptibility-weighted contrast-enhanced perfusion MRI; glioblastoma; glioma; imaging genomics; metastasis; molecular imaging; peak height; percentage of signal intensity recovery.
Conflict of interest statement
Figures
Similar articles
-
DCE and DSC MR perfusion imaging in the differentiation of recurrent tumour from treatment-related changes in patients with glioma.Clin Radiol. 2014 Jun;69(6):e264-72. doi: 10.1016/j.crad.2014.01.016. Epub 2014 Mar 1. Clin Radiol. 2014. PMID: 24594379
-
Comparison of three different MR perfusion techniques and MR spectroscopy for multiparametric assessment in distinguishing recurrent high-grade gliomas from stable disease.Acad Radiol. 2013 Dec;20(12):1557-65. doi: 10.1016/j.acra.2013.09.003. Acad Radiol. 2013. PMID: 24200483
-
Dynamic susceptibility-weighted contrast-enhanced perfusion MR imaging in pediatric patients.Neuroimaging Clin N Am. 2006 Feb;16(1):137-47, ix. doi: 10.1016/j.nic.2005.11.006. Neuroimaging Clin N Am. 2006. PMID: 16543089 Review.
-
Accuracy of percentage of signal intensity recovery and relative cerebral blood volume derived from dynamic susceptibility-weighted, contrast-enhanced MRI in the preoperative diagnosis of cerebral tumours.Neuroradiol J. 2015 Dec;28(6):574-83. doi: 10.1177/1971400915611916. Epub 2015 Oct 16. Neuroradiol J. 2015. PMID: 26475485 Free PMC article. Review.
-
Dynamic contrast-enhanced susceptibility-weighted perfusion MRI (DSC-MRI) in a glioma model of the rat brain using a conventional receive-only surface coil with a inner diameter of 47 mm at a clinical 1.5 T scanner.J Neurosci Methods. 2008 Jul 30;172(2):168-72. doi: 10.1016/j.jneumeth.2008.04.022. Epub 2008 May 2. J Neurosci Methods. 2008. PMID: 18538856
Cited by
-
Imaging Role in Diagnosis, Prognosis, and Treatment Response Prediction Associated with High-grade Glioma.J Med Signals Sens. 2024 Mar 27;14:7. doi: 10.4103/jmss.jmss_30_22. eCollection 2024. J Med Signals Sens. 2024. PMID: 38993200 Free PMC article. Review.
-
Additive antiangiogenesis effect of ginsenoside Rg3 with low-dose metronomic temozolomide on rat glioma cells both in vivo and in vitro.J Exp Clin Cancer Res. 2016 Feb 13;35:32. doi: 10.1186/s13046-015-0274-y. J Exp Clin Cancer Res. 2016. PMID: 26872471 Free PMC article.
-
Comparison among conventional and advanced MRI, 18F-FDG PET/CT, phenotype and genotype in glioblastoma.Oncotarget. 2017 Oct 4;8(53):91636-91653. doi: 10.18632/oncotarget.21482. eCollection 2017 Oct 31. Oncotarget. 2017. PMID: 29207673 Free PMC article.
-
The Value of APTw CEST MRI in Routine Clinical Assessment of Human Brain Tumor Patients at 3T.Diagnostics (Basel). 2022 Feb 14;12(2):490. doi: 10.3390/diagnostics12020490. Diagnostics (Basel). 2022. PMID: 35204583 Free PMC article.
-
AG488 as a therapy against gliomas.Oncotarget. 2017 May 30;8(42):71833-71844. doi: 10.18632/oncotarget.18284. eCollection 2017 Sep 22. Oncotarget. 2017. PMID: 29069750 Free PMC article.
References
-
- Omuro A1, DeAngelis LM. Glioblastoma and other malignant gliomas: a clinical review. JAMA. 2013;310(17):1842–1850. - PubMed
-
- Aronen HJ, Gazit IE, Louis DN, et al. Cerebral blood volume maps of gliomas: comparison with tumor grade and histologic findings. Radiology. 1994;191:41–51. - PubMed
-
- Knopp EA, Cha S, Johnson G, et al. Glial neoplasms: dynamic contrast-enhanced T2*-weighted MR imaging. Radiology. 1999;211:791–798. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical