

Cor pulmonale parvus in chronic obstructive pulmonary disease and emphysema: the MESA COPD study
- PMID: 25440095
- PMCID: PMC4347835
- DOI: 10.1016/j.jacc.2014.07.991
Cor pulmonale parvus in chronic obstructive pulmonary disease and emphysema: the MESA COPD study
Abstract
Background: The classic cardiovascular complication of chronic obstructive pulmonary disease (COPD) is cor pulmonale or right ventricular (RV) enlargement. Most studies of cor pulmonale were conducted decades ago.
Objectives: This study sought to examine RV changes in contemporary COPD and emphysema using cardiac magnetic resonance (CMR) imaging.
Methods: We performed a case-control study nested predominantly in 2 general population studies of 310 participants with COPD and control subjects 50 to 79 years of age with ≥10 pack-years of smoking who were free of clinical cardiovascular disease. RV volumes and mass were assessed using magnetic resonance imaging. COPD and COPD severity were defined according to standard spirometric criteria. The percentage of emphysema was defined as the percentage of lung regions <-950 Hounsfield units on full-lung computed tomography; emphysema subtypes were scored by radiologists. Results were adjusted for age, race/ethnicity, sex, height, weight, smoking status, pack-years, systemic hypertension, and sleep apnea.
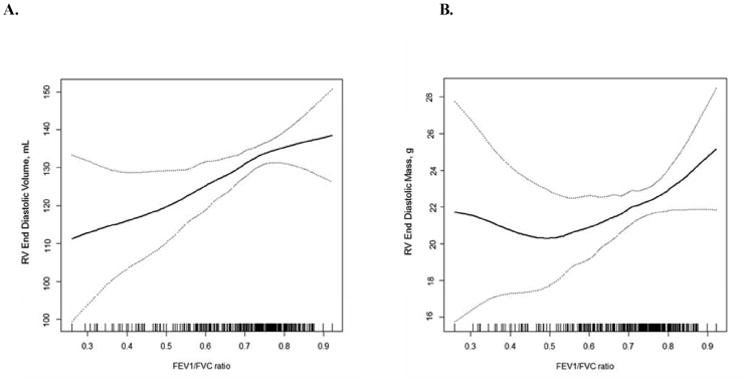
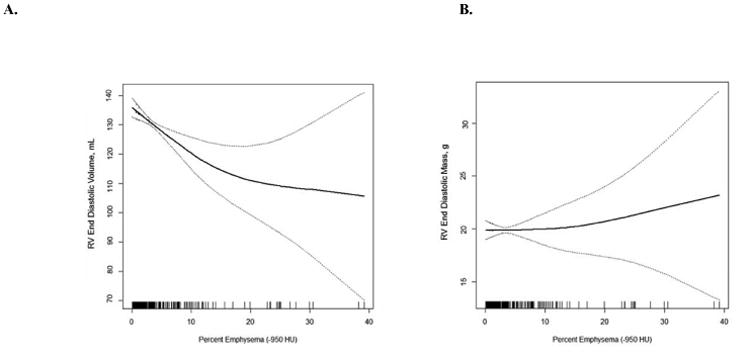
Results: Right ventricular end-diastolic volume (RVEDV) was reduced in COPD compared with control subjects (-7.8 ml; 95% confidence interval: -15.0 to -0.5 ml; p = 0.04). Increasing severity of COPD was associated with lower RVEDV (p = 0.004) and lower RV stroke volume (p < 0.001). RV mass and ejection fraction were similar between the groups. A greater percentage of emphysema also was associated with lower RVEDV (p = 0.005) and stroke volume (p < 0.001), as was the presence of centrilobular and paraseptal emphysema.
Conclusions: RV volumes are lower without significant alterations in RV mass and ejection fraction in contemporary COPD, and this reduction is related to the greater percentage of emphysema on computed tomography.
Keywords: end-diastolic volume; heart failure; pulmonary hypertension; right ventricle.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Cor pulmonale parvus: patting the elephant.J Am Coll Cardiol. 2014 Nov 11;64(19):2010-2. doi: 10.1016/j.jacc.2014.09.006. Epub 2014 Nov 3. J Am Coll Cardiol. 2014. PMID: 25440096 No abstract available.
References
-
- Hoyert DL, Xu J. Deaths: Preliminary data for 2011. Natl Vital Stat Rep. 2012;61:1–65. - PubMed
-
- Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187:347–365. - PubMed
-
- MacNee W. Pathophysiology of cor pulmonale in chronic obstructive pulmonary disease. Part one Am J Respir Crit Care Med. 1994;150:833–852. - PubMed
-
- Heath D, Brewer DB, Hicken P. Cor pulmonale in emphysema; mechanisms and pathology. Springfield, Ill.: C. C. Thomas; 1968.
-
- Kessler R, Faller M, Weitzenblum E, et al. “Natural history” of pulmonary hypertension in a series of 131 patients with chronic obstructive lung disease. Am J Respir Crit Care Med. 2001;164:219–224. - PubMed
Publication types
MeSH terms
Grants and funding
- R01-HL086719/HL/NHLBI NIH HHS/United States
- UL1-RR024156/RR/NCRR NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- R01-HL077612/HL/NHLBI NIH HHS/United States
- P30 DK054759/DK/NIDDK NIH HHS/United States
- K24 HL103844/HL/NHLBI NIH HHS/United States
- R01-HL075476/HL/NHLBI NIH HHS/United States
- R01 HL112986/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- R01-HL093081,/HL/NHLBI NIH HHS/United States
- UL1 RR024156/RR/NCRR NIH HHS/United States
- R01 HL093081/HL/NHLBI NIH HHS/United States
- K24-HL103844/HL/NHLBI NIH HHS/United States
- N01-HC95159-HC95169/HC/NHLBI NIH HHS/United States
- R01 HL086719/HL/NHLBI NIH HHS/United States
- R01 HL075476/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
