

Differences between murine and human sepsis
- PMID: 25440115
- PMCID: PMC7856627
- DOI: 10.1016/j.suc.2014.08.001
Differences between murine and human sepsis
Abstract
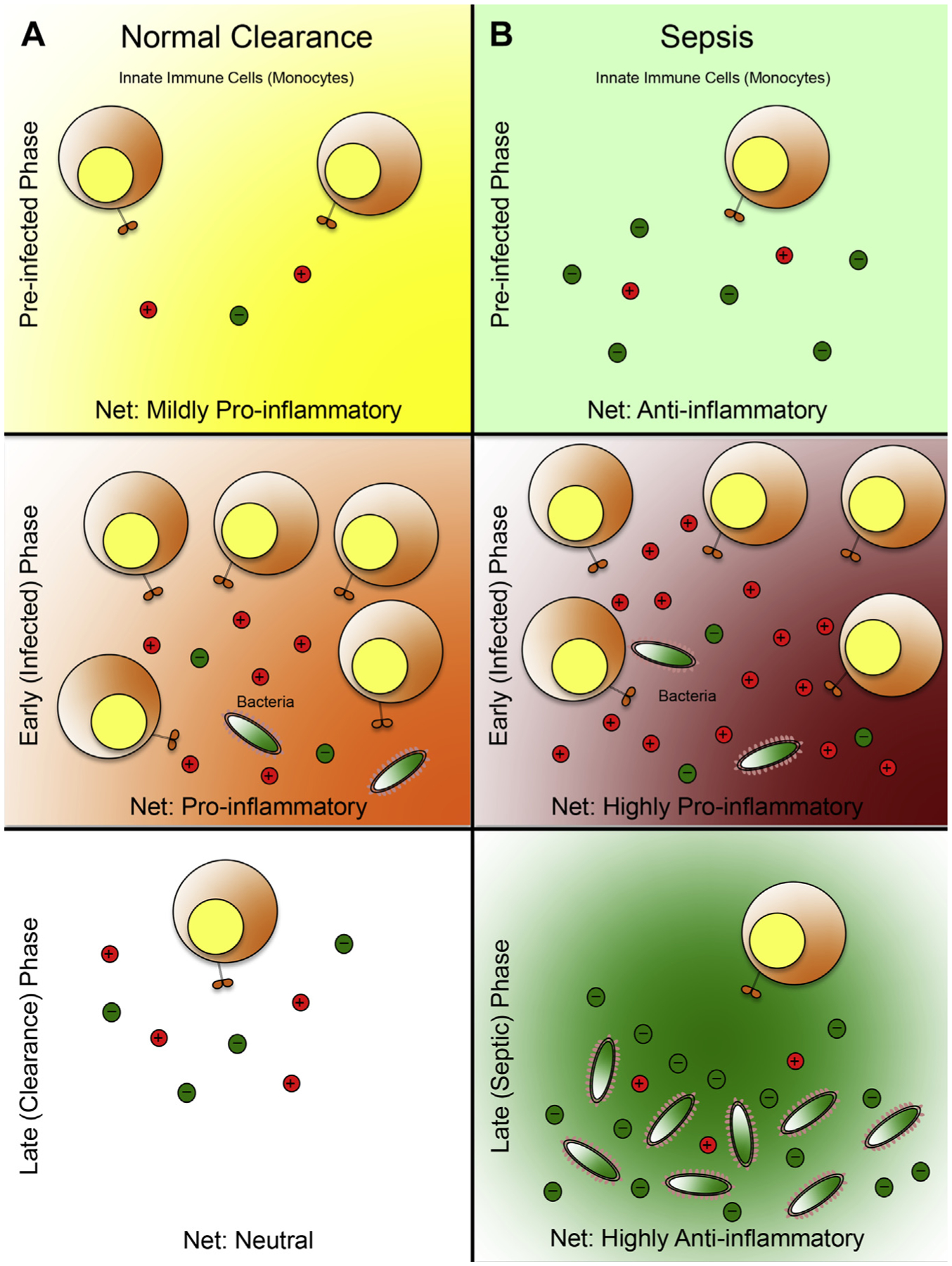
Sepsis can be defined as a systemic inflammatory response syndrome occurring in the presence of an infectious source. Over the past 25 years, numerous guidelines have been established to clarify definitions and improve the overall management of clinical sepsis. In light of these multiple paradigm shifts, this review attempts to summarize the innate immunologic alterations that manifest during sepsis, establish and compare mouse models of sepsis with the clinical course, and discuss the authors' views on additional elements that should be considered in modeling and predicting clinical sepsis from the standpoint of a basic research setting.
Keywords: Anti-inflammatory; Cytokines; Leukocytes; Proinflammatory; Sepsis; Systemic inflammatory response syndrome.
Crown Copyright © 2014. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001;29(7):1303–10. - PubMed
-
- HCUP Facts and Figures, 2006. Statistics on hospital-based care in the United States. Rockville (MD): Agency for Healthcare Research and Quality (US), 2008. - PubMed
-
- Funk DJ, Parrillo JE, Kumar A. Sepsis and septic shock: a history. Crit Care Clin 2009;25(1):83–101, viii. - PubMed
-
- LaRosa SP, Opal SM. Sepsis strategies in development. Clin Chest Med 2008; 29(4):735–47, x–xi. - PubMed
-
- Opal SM, Garber GE, LaRosa SP, et al. Systemic host responses in severe sepsis analyzed by causative microorganism and treatment effects of drotrecogin alfa (activated). Clin Infect Dis 2003;37(1):50–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
