

Visceral adiposity and the risk of metabolic syndrome across body mass index: the MESA Study
- PMID: 25440591
- PMCID: PMC4268163
- DOI: 10.1016/j.jcmg.2014.07.017
Visceral adiposity and the risk of metabolic syndrome across body mass index: the MESA Study
Abstract
Objectives: This study sought to evaluate differential effects of visceral fat (VF) and subcutaneous fat and their effects on metabolic syndrome (MetS) risk across body mass index (BMI) categories.
Background: The regional distribution of adipose tissue is an emerging risk factor for cardiometabolic disease, although serial changes in fat distribution have not been extensively investigated. VF and its alterations over time may be a better marker for risk than BMI in normal weight and overweight or obese individuals.
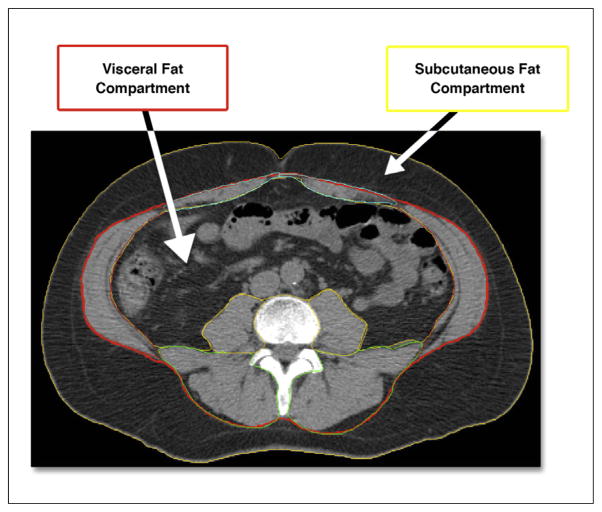
Methods: We studied 1,511 individuals in the MESA (Multi-Ethnic Study of Atherosclerosis) with adiposity assessment by computed tomography (CT). A total of 253 participants without MetS at initial scan underwent repeat CT (median interval 3.3 years). We used discrete Cox regression with net reclassification to investigate whether baseline and changes in VF area are associated with MetS.
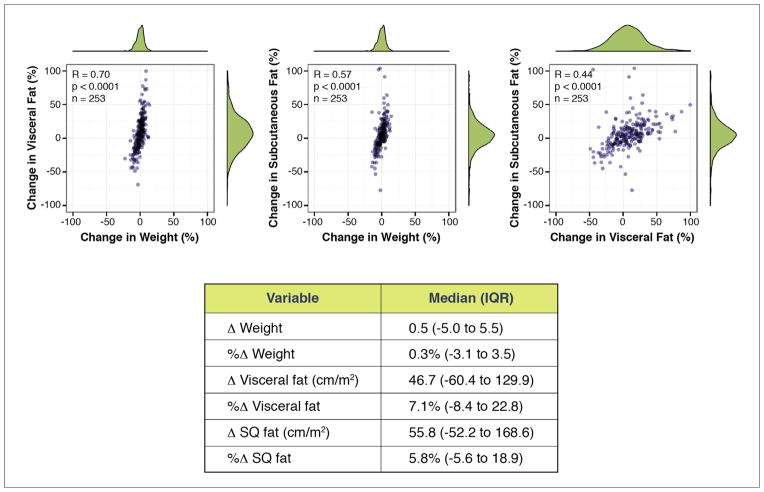
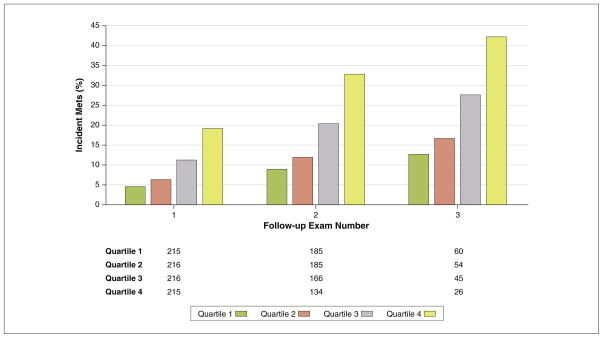
Results: Higher VF was associated with cardiometabolic risk and coronary artery calcification, regardless of BMI. After adjustment, VF was more strongly associated with incident MetS than subcutaneous fat regardless of weight, with a 28% greater MetS hazard per 100 cm(2)/m VF area and significant net reclassification (net reclassification index: 0.44, 95% confidence interval [CI]: 0.29 to 0.60) over clinical risk. In individuals with serial imaging, initial VF (hazard ratio: 1.24 per 100 cm(2)/m, 95% CI: 1.08 to 1.44 per 100 cm(2)/m, p = 0.003) and change in VF (hazard ratio: 1.05 per 5% change, 95% CI: 1.01 to 1.08 per 5% change, p = 0.02) were associated with MetS after adjustment. Changes in subcutaneous fat were not associated with incident MetS after adjustment for clinical risk and VF area.
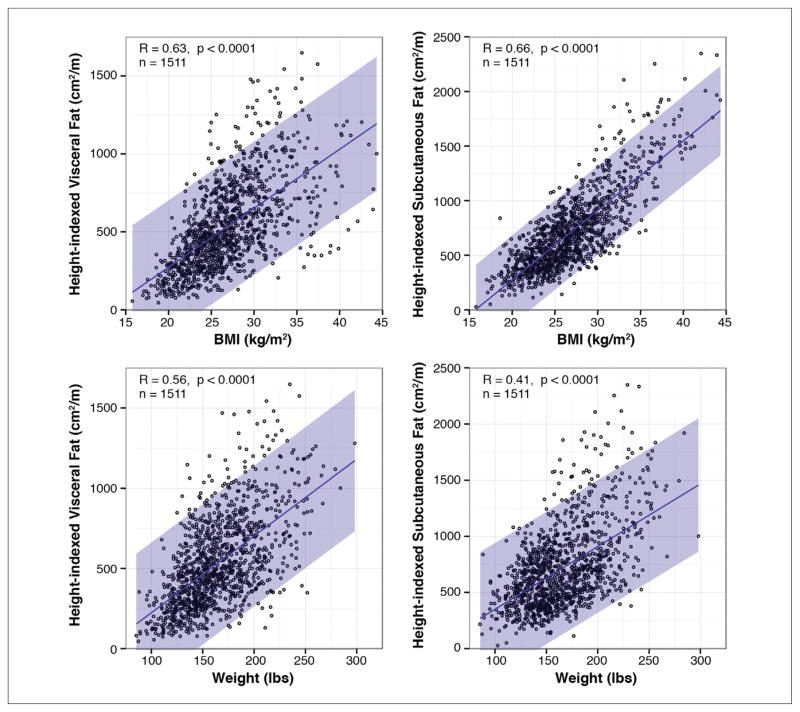
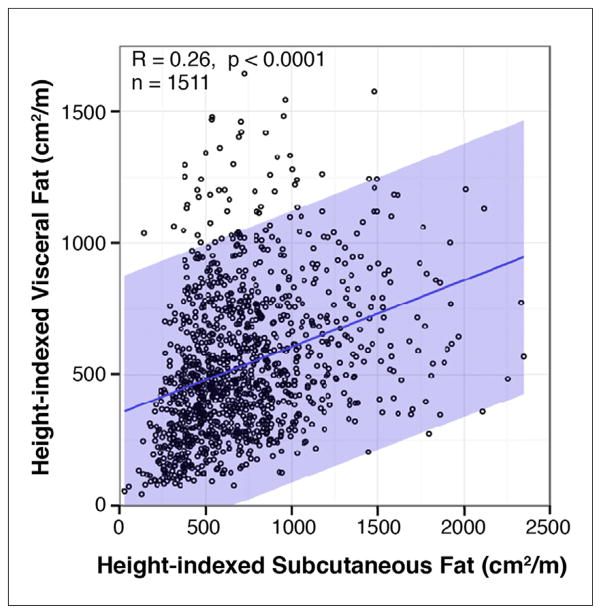
Conclusions: VF is modestly associated with BMI. However, across BMI, a single measure of and longitudinal change in VF predict MetS, even accounting for weight changes. Visceral adiposity is essential to assessing cardiometabolic risk, regardless of age, race, or BMI, and may serve as a marker and target of therapy in cardiometabolic disease.
Keywords: cardiometabolic risk; metabolic syndrome; obesity.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Separating the VAT from the FAT: new insights into the cardiometabolic risks of obesity.JACC Cardiovasc Imaging. 2014 Dec;7(12):1236-8. doi: 10.1016/j.jcmg.2014.08.007. JACC Cardiovasc Imaging. 2014. PMID: 25496542 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
