

Real-time use of instantaneous wave-free ratio: results of the ADVISE in-practice: an international, multicenter evaluation of instantaneous wave-free ratio in clinical practice
- PMID: 25440803
- PMCID: PMC4220017
- DOI: 10.1016/j.ahj.2014.06.022
Real-time use of instantaneous wave-free ratio: results of the ADVISE in-practice: an international, multicenter evaluation of instantaneous wave-free ratio in clinical practice
Abstract
Objectives: To evaluate the first experience of real-time instantaneous wave-free ratio (iFR) measurement by clinicians.
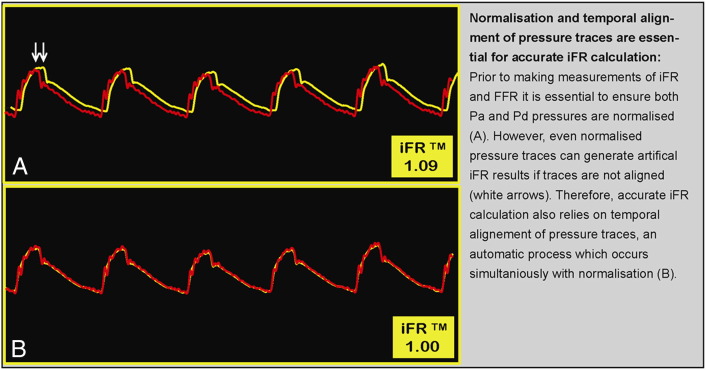
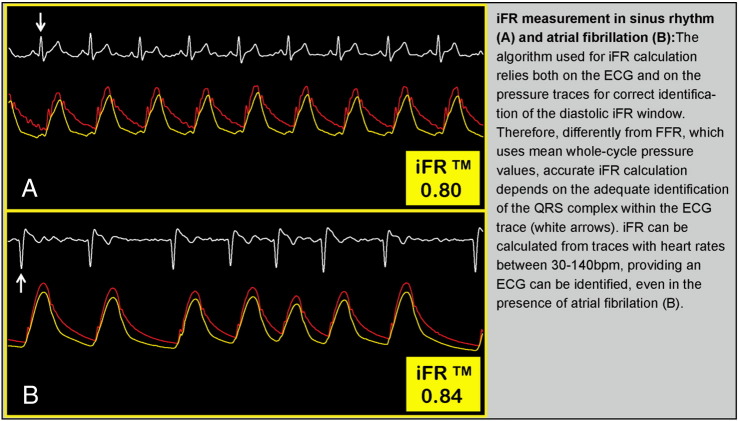
Background: The iFR is a new vasodilator-free index of coronary stenosis severity, calculated as a trans-lesion pressure ratio during a specific period of baseline diastole, when distal resistance is lowest and stable. Because all previous studies have calculated iFR offline, the feasibility of real-time iFR measurement has never been assessed.
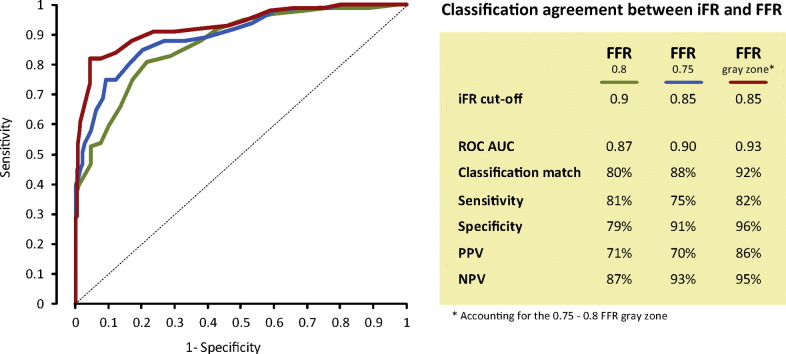
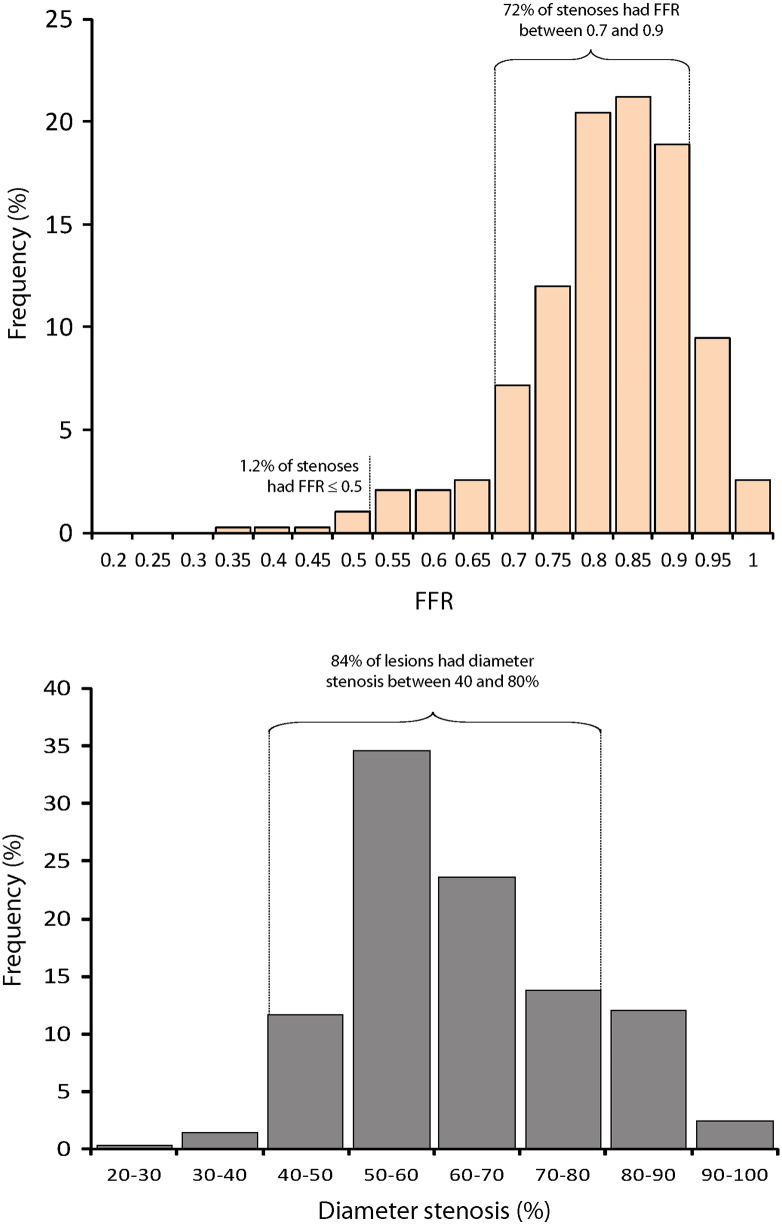
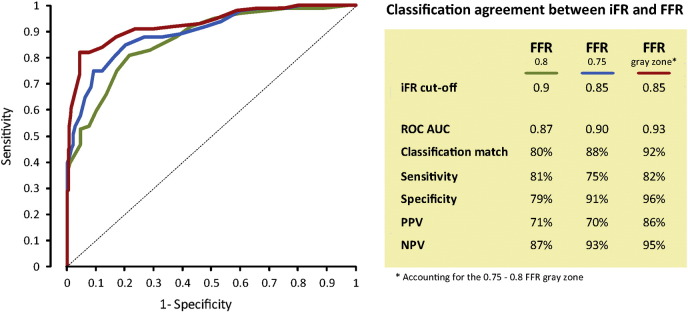
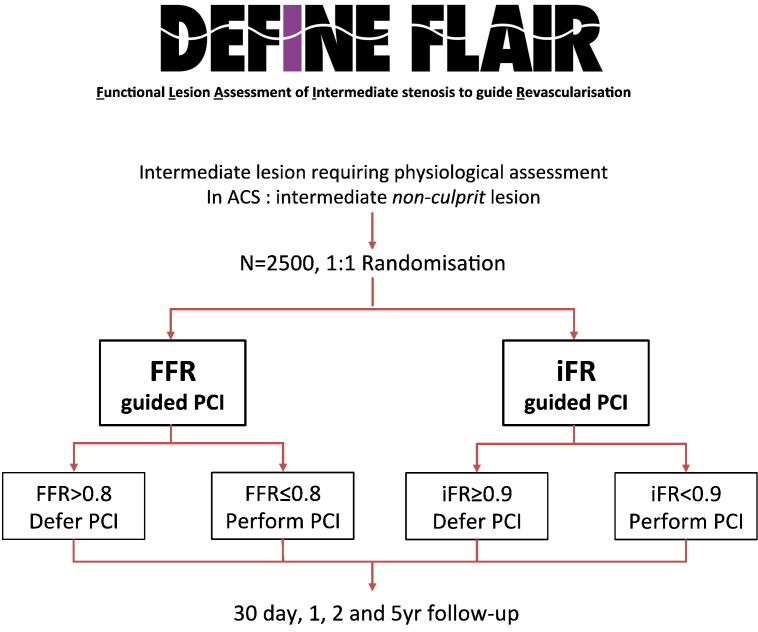
Methods: Three hundred ninety-two stenoses with angiographically intermediate stenoses were included in this multicenter international analysis. Instantaneous wave-free ratio and fractional flow reserve (FFR) were performed in real time on commercially available consoles. The classification agreement of coronary stenoses between iFR and FFR was calculated.
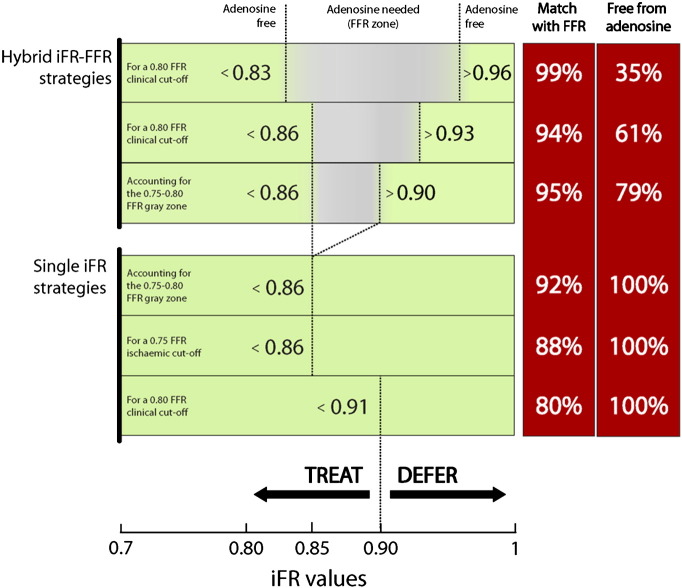
Results: Instantaneous wave-free ratio and FFR maintain a close level of diagnostic agreement when both are measured by clinicians in real time (for a clinical 0.80 FFR cutoff: area under the receiver operating characteristic curve [ROC(AUC)] 0.87, classification match 80%, and optimal iFR cutoff 0.90; for a ischemic 0.75 FFR cutoff: iFR ROC(AUC) 0.90, classification match 88%, and optimal iFR cutoff 0.85; if the FFR 0.75-0.80 gray zone is accounted for: ROC(AUC) 0.93, classification match 92%). When iFR and FFR are evaluated together in a hybrid decision-making strategy, 61% of the population is spared from vasodilator while maintaining a 94% overall agreement with FFR lesion classification.
Conclusion: When measured in real time, iFR maintains the close relationship to FFR reported in offline studies. These findings confirm the feasibility and reliability of real-time iFR calculation by clinicians.
Copyright © 2014 The Author. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Sen S., Escaned J., Malik I.S. Development and validation of a new adenosine-independent index of stenosis severity from coronary wave-intensity analysis: results of the ADVISE (ADenosine Vasodilator Independent Stenosis Evaluation) study. J Am Coll Cardiol. 2012;59(15):1392–1402. - PubMed
-
- Petraco R., Escaned J., Sen S. Classification performance of instantaneous wave–free ratio (iFR) and fractional flow reserve in a clinical population of intermediate coronary stenoses: results of the ADVISE registry. Eurointervention. 2013;9(1):91–101. - PubMed
-
- Park J.J., Petraco R., Nam C.W. Clinical validation of the resting pressure parameters in the assessment of functionally significant coronary stenosis; results of an independent, blinded comparison with fractional flow reserve. Int J Cardiol. 2013;168(4):4070–4075. - PubMed
-
- Jeremias A., Maehara A., Genereux P. Multicenter core laboratory comparison of the instantaneous wave–free ratio and resting P/P with fractional flow reserve: the RESOLVE study. J Am Coll Cardiol. 2013;63(13):1253–1261. - PubMed
-
- Sen S., Asrress K.N., Nijjer S. Diagnostic classification of the instantaneous wave–free ratio is equivalent to fractional flow reserve and is not improved with adenosine administration: results of CLARIFY (Classification Accuracy of Pressure-Only Ratios Against Indices Using Flow Study) J Am Coll Cardiol. 2013;61(13):1409–1420. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
